 Home
Home
|
Table of Content - Volume 20 Issue 3 - December 2021
A study on morphology of infra renal inferior vena cava in Jharkhand population
Tutor, Department of Anatomy, Phulo Jhano Medical College, Dumka, Jharkhand, INDIA. Email: keshavkrishna234@gmail.com
Abstract Background: Inferior Vena Cava (IVC) is formed by a complex process during embryogenesis. Most common anomaly seen is double inferior vena cava followed by the right sided vena cava. Knowledge of morphology and variations of infra renal segment of IVC and its tributaries is important while doing surgical/ orthopaedic procedures such as renal transplant and anterior approach to lumbar vertebrae. Anomalies of IVC may cause hydronephrosis, ureteral stenosis, and recurrent urinary tract infections. Thus, considering the applied importance of morphology of infra renal IVC, the present study was undertaken in relation to the local population of Jharkhand. Aim and Objectives: To elucidate the variations in morphology and morphometry of cadaveric infra renal inferior vena cava viz. its level of origin, diameter, length and tributaries in the population of Jharkhand, India. Material and Methods: Instruments: dissecting instruments, slide calliper. Method: Retroperitoneal structures were dissected to expose IVC, and its tributaries. Origin of IVC, infra renal portion of IVC, renal veins and lumbar veins were observed, right gonadal vein was traced to its drainage into the IVC, and measurements were taken. Results and Discussion: - Level of IVC formation-: L5- 40%, junction of L4 and L5- 20%, L4- 40%. Average values of measurements of IVC: Length of infra renal segment of IVC- 10.02 cm. Diameter at origin- 1.47cm. The level of drainage of renal veins: right- junction of L3-L4 to T12, left- L3 to junction between T12-L1. Conclusion: The present study, conducted at RIMS, Ranchi, Jharkhand, reiterates the concept that anomalies of IVC is uncommon. Results of this study will help the clinicians, radiologists, general and orthopaedic surgeons in diagnosing and managing anomalies/diseases of the retro peritoneal area in local population of Jharkhand. It will also be helpful in routine classroom discussions and dissection. Key Words: Infra renal Inferior Vena Cava, Morphology
INTRODUCTION The inferior vena cava (IVC), drains from all the structures below the diaphragm (including the diaphragm) except the viscera drained by the portal vein.1,2,3 It is formed by union of common iliac veins, anterior to middle third of fifth lumbar vertebral body, approximately 2.5 cm to the right of median plane.1 It ascends anterior to the vertebral column to the right of aorta. Its tributaries are 3rd and 4th lumbar veins on each side, right gonadal vein, renal veins, right supra renal vein. The infra-hepatic segment is derived from changes in three parallel sets of veins, viz., the post-cardinal, sub-cardinal and supra-cardinal veins. The IVC is formed from below upwards by the confluence of the common iliac veins, a short segment of the post-cardinal vein, the post-cardinal and supra-cardinal anastomoses, part of right supracardinal vein, the right supra-cardinal and sub-cardinal anastomosis, right sub-cardinal vein, a new anastomotic channel of double origin (the hepatic segment of inferior vena cava), and the cardiac termination of the right vitelline hepato-cardiac vein (common hepatic vein).1,2 This complicated arrangement may result in many variations/anomalies, such as those of length, location, abnormal connections, drainage, absence or duplication. It is sometimes replaced, below the level of renal veins, by two more or less symmetrical vessels, often associated with the failure of interconnection between the common iliac veins, and persistence on the left of a longitudinal channel (usually the supra-cardinal or sub-cardinal vein) that normally disappears in early foetal life. In complete visceral transposition, the inferior vena cava lies to the left of the aorta. Variations of IVC were first described by Abernethy in 1973 in a 10-month-old child with polysplenia and dextrocardia and congenital mesocaval shunt with continuation of IVC into the azygous vein (continuous azygous).12 Duplicated IVC, the most common type of variation was described first in 1916 in the Gross Anatomy Laboratory in London.13 The incidence of variations of inferior vena cava (IVC) ranges from 0.4 to 4%.7 When the incidence of IVC variation is combined with variations of left renal vein and superior vena cava variation the total incidence is up to 8.7 % [8]. Saad KR et al. cited it to range from 0.4 to 4%.6 Chen Huayue et al. quoted the incidence of variation to range from 0.3% to 3 %.9 They have analysed 109 cases of IVC anomalies published in the literature from 1967 to 2011. Most common variation of inferior vena cava is double (duplicate) IVC. Incidence of double (duplicate) IVC ranges from 0.2% to 3%.10 The second most common variation encountered is left sided IVC. Incidence of left sided IVC is 0.69%.10 When these anatomical variations cause illness and symptoms, they are considered as anomaly.11 Prior to the modern radiological era, variations of IVC were observed during routine cadaveric dissection in gross anatomy courses and during post mortem examination. Now in the present era with the advent of advanced imaging techniques, more and more numbers and types of IVC variations are being reported. Phlebography is another radiological technique which is considered by many authors to be the Gold Standard for the diagnosis of Double IVC, the most common type of variation reported. Many of the cases of infra renal IVC variations are asymptomatic and are clinically silent. Yet these variations have very important clinical implications. Ignorance of these variations may result in radiological misdiagnosis. As for example, Double IVC may be misdiagnosed as a retroperitoneal lymphadenopathy, a retroperitoneal cyst or an aneurysm on radiography, leading to unnecessary intervention. Knowledge of variations of IVC and its tributaries are of paramount importance while performing kidney transplant surgeries. IVC filters are placed for thromboembolic diseases. There may be recurrent thromboembolic phenomenon if there is duplicate IVC, which is not diagnosed prior to the procedure and the filter is placed in only one of the two IVC. Similarly, it would be difficult to place filter in left sided IVC through a trans-jugular approach. Knowledge of variations of IVC is important while performing less invasive, orthopaedic anterior lumbar inter body fusion. These procedures are being routinely taken up in various tertiary care facilities and institutions. Venous injury is also more common due to its intimate contact with the vertebral column and is also more difficult to manage than an arterial injury.1 Duplicate IVC may cause hydronephrosis of left kidney. Duplicated IVC may be present anterior to aorta at the level of coeliac trunk, compressing it and causing post prandial abdominal pain. Retro-caval ureter which occurs exclusively on the right side may cause ureteral stenosis, upstream hydro nephrosis and recurrent urinary tract infections. Agenesis of IVC is a risk factor for Deep Vein Thrombosis (DVT) due to stasis of blood in the veins, accounting for about 5% of cases of DVT in young patients. Thus, considering the applied importance of morphology of infra renal IVC, the present study was undertaken in relation to the local population of Jharkhand. AIM AND OBJECTIVES: The present study was aimed to elucidate the variations in morphology of cadaveric infra renal inferior vena cava viz., vertebral level of origin, length, diameter at origin, relation to surrounding structures and tributaries, in the local population of Jharkhand. The formative, renal, right gonadal, lumbar, and suprarenal tributaries were studied with respect to their vertebral level of drainage, their number (including supernumerary veins if any) and other factors.
MATERIAL AND METHOD The study was done on 10 adults dissected human infra renal IVC of both sexes, over a period of about one and a half year on ten embalmed adult cadavers during routine dissection in the dissection hall of Department of Anatomy, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand. Inferior Vena Cava was exposed with the help of scalpel, scissors and forceps, using the standard dissecting technique. In this study following details of the infra renal IVC were recorded: Origin- vertebral level, site, position, diameter and formative tributaries. Length, course and relations. Tributaries. The land mark used for counting the vertebra was sacral promontory. Length and diameter were measured using string, divider, scale, measuring tape and slide calliper. Length of infra renal portion of inferior vena cava was measured from its origin to the point of drainage of that renal vein which was placed more inferiorly.
RESULTS Diameter of IVC at origin ranged from 1.02 cm to 1.66 cm, the mean value 1.47 cm and standard deviation 0.19 cm. Total Length of Inferior Vena Cava ranged from 19.7 cm to 24.73 cm. This seemed to correlate with the height of the individual specimen under study. Average length of inferior vena cava was observed to be 21.87 cm. The average length of infra renal segment was 10.02 cm, median value was 10.1 cm, S.D. was calculated to be 1.85 while the range of length was 6 cm to 12.6 cm. Formative tributaries in all the ten cadavers were the right and left common iliac veins at the vertebral level of L4, L4-L5 or L5 vertebra, slightly to the right of median plane and just below, behind and slightly to the right of bifurcation of abdominal aorta. The right common iliac artery was observed to be in anterior relation to the right common iliac vein and origin of inferior vena cava. Left common iliac artery was in anterior relation to left common iliac vein. Level of drainage of left renal vein into inferior vena cava were observed to be anywhere between L3 to junction between T12-L1 vertebrae. It was at the level of L1 in five cadavers, at the level of L1-L2 in two cadavers, at level of T12 in one cadaver, at the level of junction between T12-L1 in one cadaver and at the level of L3 in one cadaver. Length between the origin of inferior vena cava and the point of drainage of left renal vein varied from 7 cm to 12.6 cm, with an average value of 10.62 cm and S.D. of 1.90. Variations, such as double renal veins, two renal veins uniting to form single renal vein, renal collar or retro aortic left renal vein were not observed in any of the dissected cadavers. Lumbar veins- An average of 3 lumbar veins on left side, and 2 lumbar veins on right side drained into inferior vena cava. Of all the 42 lumbar veins draining into inferior vena cava in various cadavers 22 veins were paired (i.e., a total of 11 pairs), while rest 20 of it were unpaired. In all the cadaver, right gonadal vein drained directly into the inferior vena cava, slightly below the level of drainage of right renal veins and left gonadal vein drained into the left renal vein. Duplication of gonadal vein was not observed.
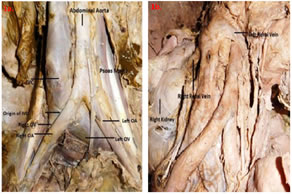
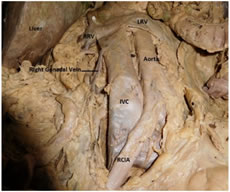
Figure 1 Figure 2 Figure 1: Origin and Infra-renal segment of IVC(1a: Origin of IVC, 1b: Right Renal Vein draining into IVC) Figure 2: Right gonadal vein draining into IVC
DISCUSSION In the present study IVC formed at L5 vertebral level in 40% of cadavers, at junction of L4 and L5 in 20% of cadavers, while at level of L4 vertebrae in rest 40% of cadavers. The level of inferior vena cava formation extends from as high as L3-L4 lumbar disc to L5-S1 intervertebral disc. But most common position is anywhere between body of L4 to body of L5. The variability of the iliocaval confluence is high and complicates the anterior approach to the lumbosacral spine. The cause for this difference in observations may be because of two reasons. One reason could be the difference in the population under study. The venous anatomy elsewhere in the body too is normally highly variable one.
Table 1: Comparison of Vertebral levels of formation of IVC
In the present study the average length of infra renal segment of IVC was 10.02 cm ± 1.85 cm and its range was from 6cm to 12.6 cm. This was comparable with other such studies.
Table 2: Comparison of length of infra renal segment of IVC
The diameter of IVC at its origin ranged from 1.02 cm to 1.66 cm with an average value of 1.47 cm, which was similar to other such study. Table 4: Comparison of diameter of Infra Renal Segment of IVC
In all the cadavers the formative tributaries were right and left common iliac veins. Variation or anomaly of any type was not observed. In the present study the right renal vein opened into the IVC at the level of L1 vertebrae in 30% of cases and at L2 vertebrae in other 30% of cases, while on the left side 40% of renal veins drained at the level of L1 vertebrae. The lowest level of drainage of renal veins was observed for the right renal vein at the level of L3-L4. While the highest level of drainage was observed at T12 level, on right and left side in two and one cadaver respectively. The incidence of right hepatic veins draining separately into IVC in the reported literature has varied from 83% to 90%. The incidence of common ostia draining left and middle hepatic vein in various literatures has varied from 70% to 88%. Incidence of paired lumbar veins was 52% while that of unpaired was 48% in the present study. In one study the incidence of unpaired lumbar veins was 62%, while in the present study the incidence of paired and unpaired lumbar veins is almost equal. The knowledge of lumbar veins and their variations is important while carrying out surgeries on the lumbar vertebra through anterior approach.
CONCLUSION Variations in morphology of IVC has been documented since long. Present study reaffirms the notion that anomalies of inferior vena cava and its tributaries are rare, while variations may be present. This can be of help to surgeons and clinicians while planning and performing various surgical procedures such as hepatic and renal transplantation, segmental resection of liver, and placement of filter in inferior vena cava when there is recurrent episode of deep vein thrombosis, etc. in local population of Jharkhand.
REFERENCES
Policy for Articles with Open Access
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.