 Home
Home
|
Table of Content - Volume 21 Issue 1 - January 2022
Anomalous lumbricals in and around the carpal tunnel and its clinical implications- Cadaveric study
Professor, Department of Anatomy, Varun Arjun Medical College and Rohilkhand Hospital, Banthra-Shahjahanpur - 242307, Uttar Pradesh, INDIA. Email: kalyankosuric@gmail.com
Abstract Background: The anatomical variations and abnormalities of the muscles of the upper limb are not uncommon; their importance becomes apparent with regard to surgical approaches for various clinical conditions involving the upper limb especially lumbricals. The lumbricals of the upper limb are four small muscles resembling the shape of earthworm and play a vital role in precision movements of the hand. Aim:Accordingly, the aim of this study was designed to evaluate the prevalence of anatomical variations of lumbricals in and around the carpal tunnel. Methods and Materials: This study was carried out on routine human cadaveric dissection of upper limbs (Between 2010-2021) for medical undergraduates. Dissections were performed on a body that had been donated for the purpose of medical education and research to the laboratory of anatomy in accordance with the institutional ethical standards and Indian anatomy act. Anatomical variations of lumbricals in and around the carpal tunnel were observed and photographs were taken for proper documentation. Results: Out of 150 upper limbs of 75 formalin embalmed human cadavers (43-male and 32- female), in 10 cadavers following anatomical variations were observed- 1. In seven male cadavers all lumbricals of the right-hand showed higher origin, proximal to the flexor retinaculum in the lower anterior part of the forearm with unipennate fourth lumbrical; 2. In one female cadaver all unipennate lumbricals of the right hand with higher origin, proximal to the flexor retinaculum in the lower anterior part of the forearm with congenital absence of flexor digitorum profundus tendon of little finger were noted; 3. In two cadavers (one male and one female) multiple anomalous bulky lumbricals with higher origin were noted. To the best of knowledge such anomalous lumbrical muscles in and around the carpal tunnel has not been cited in the recent medical literature. All the lumbrical muscles found in and around the carpal tunnel in the present study can increase the pressure over the median nerve and may cause carpal tunnel syndrome. Awareness of these variations is necessary to avoid complications during various radio diagnostic procedures or surgeries in the hand. Key Words: Camptodactyly, carpal tunnel syndrome, hypertrophic, lumbricals.
INTRODUCTION The flexor digitorum profundus (FDP) is a bulkiest muscle of the forearm and takes origin from the interosseous membrane, coronoid and olecranon process, upper three-fourths of posterior boarder and shaft of ulna. The muscle below forms four tendons, passes deep to the flexor retinaculum and inserted to the palmar surface of the base of the distal phalanx of the medial four fingers (index, middle, ring, and little fingers). It flexes the metacarpophalangeal and distal interphalangeal joints of medial four fingers. It also acts as a flexor of the wrist, and proximal interphalangeal joints of medial four fingers along with flexor digitorum superficialis (FDS). The lumbricals are four small, worm-like intrinsic muscles of hand arise from the four tendons of FDP and are inserted into the dorsal digital expansion of the medial four fingers. They are numbered from the lateral to the medial side. First and second lumbricals are unipennate and originate from the radial side of the FDP of the index and middle finger. Third and fourth lumbrical are bipinnate arise from the adjacent sides of the FDP tendons for of the middle, ring and little fingers. All lumbricals inserted into the radial side of dorsal digital expansion of the medial four fingers. Through the dorsal digital expansion, they insert in to the dorsal surface of the base of the middle and distal phalanges. Thus, they act as link muscles since they connect the deep flexor tendons to the extensor tendons of the fingers. Carpal tunnel is a narrow osseo-fibrous passageway found on the anterior portion of wrist. It serves as the entrance to the palm for median nerve, tendons of flexor digitorum superficialis, flexor digitorum profundus and flexor pollicis longus. Anomalous or abnormal structures in and around the carpal tunnel may increase the volume of carpal tunnel which may results in compression of median nerve. Compression of median nerve within the carpal tunnel is called as carpal tunnel syndrome, and is manifested by weakness and wasting of the thenar muscles with loss of power of opposition, and loss of cutaneous sensation of the palmar surface of lateral three and half of the digits. Thus, knowledge of the existence of anomalous or abnormal structures in and around the carpal tunnel as well as the location of compression is useful in determining the pathology and appropriate treatment for compressive neuropathies. Accordingly, the aim of this study was designed to evaluate the prevalence of anomalous origin of lumbricals in and around the carpal tunnel.
MATERIALS AND METHODS This study was carried out on150 upper limbs (Between 2010-2021) of 75 formalin embalmed human cadavers (43 male and 32 female) for medical undergraduates. Dissections were performed on a body that had been donated for the purpose of medical education and research to the laboratory of anatomy in accordance with the institutional ethical standards and Indian anatomy act. Anatomical variations of lumbricals in relation to in and around carpal tunnel were observed and photographs were taken for proper documentation.
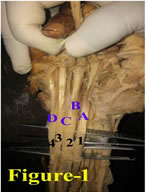
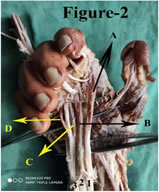
RESULTS Out of 150 upper limbs of 75 formalin embalmed human cadavers the following congenital variations of lumbricals were noted- In seven middle aged male cadavers all right-handed lumbrical muscles were arising from the tendons of FDP, proximal to the flexor retinaculum in the lower anterior part of the forearm and extending in to then palm through carpal tunnel. Fourth lumbrical was noted as unipennate, arising from the radial side of FDP tendon of little finger. (Figure-1) In one middle-aged female cadaver all right-handed lumbrical muscles were arising from the tendons of FDP, proximal to the flexor retinaculum in the lower anterior part of the forearm and extending in to then palm through carpal tunnel. All lumbricals were noted as unipennate, with congenital absence of FDP tendon of little finger. Third and fourth lumbricals are arising from the respective sides of FDP tendon of ring finger. (Figure-2) In left upper extremity of one male cadaver bulky (hypertrophied) second and third lumbricals were noted in the carpal tunnel, and fourth lumbrical origin was noted in the lower anterior part of forearm proximal to the flexor retinaculum. Second lumbrical was noted as bipinnate arising from the palmar side of FDP tendon of middle finger and radial side of FDP tendon of ring finger. Third lumbrical was noted as unipennate arising from the radial side of FDP tendon of ring finger. (Figure-3) In left upper extremity of one female cadaver bulky (hypertrophied) second, third and fourth lumbricals were arising in the carpal tunnel from the tendons of FDP. First lumbrical was bipinnate arising from the radial side of FDS and FDP tendons of index finger. (Figure-4 and Figure-5) Figure 1 Figure 2 Figure 1: Showing higher origin (in the lower part of forearm) of anomalous lumbricals in a right hand( A, B, C, D- First, second, third (bipinnate) and fourth (unipennate) lumbricals; 1, 2, 3, 4- medial four tendons of FDP); Figure 2: Showing higher origin (in the lower part of forearm) of anomalous lumbricals in a right hand with congenital absence of FDP tendon to the little finger (A, B, C, D- First, second, third (unipennate) and fourth (unipennate) lumbricals; 1, 2, 3 - tendons of FDP); Figure 3: Showing higher origin (in the lower part of forearm) of anomalous lumbricals in a left hand with congenital absence of FDP tendon of little finger (A, B, C, D- First, second (bulky bipinnate), third (bulky bipinnate) and fourth (bulky bipinnate) lumbricals; 1, 2, 3 - tendons of FDP); Figure 4: Showing anomalous lumbricals in a left hand (Yellow circle-- First lumbrical(bipinnate); 1- tendon of FDS; 2 - tendon of FDP); Figure 5: Showing higher origin of anomalous lumbricals in a left hand with anomalous muscle (Black circle- Anomalous muscle in the lower part of forearm; Black arrows- Bulky second, third and fourth lumbricals)
DISCUSSION Anatomically lumbricals take origin distal to the flexor retinaculum form the four tendons of flexor digitorum profundus muscle. Many studies reported higher origin of first and second lumbricals in the carpal tunnel. Chakravarthi et al. reported origin of all unipennate lumbricals from the four tendons of FDP muscle beneath the flexor retinaculum in the carpal tunnel of right hand of a middle-aged male cadaver. 1In another study by Tintu et al. reported two additional bellies in the right hand of a male cadaver, one additional belly for first lumbrical originated from the radial side of the tendon of FDS of the index finger and another additional belly for second lumbrical originated from the ulnar side of the tendon of FDP of the index finger, deep to the flexor retinaculum. 2 In this study, in eight cadavers (7 male and 1 female) all lumbricals were originated proximal to the flexor retinaculum in the anterior part of the forearm and extending in to then palm through carpal tunnel. Out of eight cadavers in seven male cadavers all lumbricals were found unipennate except second which is bipinnate in origin and in one female cadaver all lumbricals were found as unipennate in origin. Such higher origin of lumbricals in the anterior part of forearm proximal to the flexor retinaculum noted in this study have not seated in the modern medical literature. Benny et al. reported bilateral carpal tunnel syndrome in a 73-year-old male retired army veteran. 3 In which hypertrophied first and second lumbricals in the right hand of carpal tunnel, and abnormal ring finger lumbricals originated from the tendons of FDP and FDS in the left hand of carpal tunnel as well as in the forearm were observed. Where as in the present study in a left hand of middle-aged male cadaver, hypertrophied bipinnate first lumbrical in the carpal tunnel as well as in the forearm and hypertrophied bipinnate second and third lumbricals in the carpal tunnel were observed. Such anomalous or accessory or hypertrophic bellies in and around the carpal tunnel noted in this study may reduce the anatomical capacity of carpal tunnel and leads to carpal tunnel syndrome. Anomalous or accessory muscles or tendons in the upper limb are quite common, may lead to confusion during surgical procedures which results in errors in both diagnosis and treatment. Different accessory or anomalies or abnormal muscles of upper limb have been described in the literature. 4-7 Although many anatomical variations in the forearm were reported in the past, Chakravarthi et al.reported a rare case of an accessory muscle of forearm originated from the middle of the medial surface of the ulna, when traced distally deep to the flexor retinaculum in the carpal tunnel it merged with the tendon of the index finger of FDS. 8 In this study also a rare accessory muscle of forearm originated from the tendon of the index finger of FDP, when traced distally deep to the flexor retinaculum in the carpal tunnel it merged with the second lumbrical. As per review of literature such accessory muscle noted in this study, first of kind, have not been reported in the literature till date. Such accessory muscles may alter or interfere the biomechanics of second lumbrical and FDP muscle. Accessory muscle belly appearance in the carpal tunnel is clinically important because it may reduce the capacity or volume of narrow carpal tunnel which results in entrapment neuropathy of the medial nerve. Congenital absence of FDP tendon to the little finger is very rare and is of high clinical importance for physicians examining patients for tendon lacerations and especially for hand surgeons operating tendon injuries. Santosh et al. reported congenital bilateral absence of FDP tendon to the little finger with abnormal lumbrical insertion to the little finger. 9 Furrer et al. reported absence of the FDP tendon to the little finger of a nine-year-old boy by ultrasound and magnetic resonance imaging. 10 Kisner et al. also reported absence of the profundus tendon to the little finger on the left hand of a 15-year-old boy during surgery. 11 In another study by Yılmaz A et al. reported a double FDS tendon to the little fingers in a left forearm of a 32-year-old female cadaver, in which one tendon connected with the index finger tendon of FDP muscle and acted as the FDP tendon to the little finger. 12 Where as in the present study, absence of FDP tendon to the little finger was noted and there was no muscle or supportive tendon substituting for the flexor digitorum profundus tendon to the little finger. Moreover, unipennate third and fourth lumbricals were taken origin from the tendon of FDP of the index finger in the carpal tunnel made this study very unique. Little finger tendon of FDP only the muscle for flexion of little finger at distal interphalangeal joint, it also helps in flexion at proximal interphalangeal joints of little finger. Congenital absence of FDP of tendon of little finger noted in this study leads to loss of flexion of little finger at distal interphalangeal joint. It also leads to flexion deformity at proximal interphalangeal joints of little finger due to imbalance between the flexor and extensor forces acting upon the proximal interphalangeal joint. Such non traumatic congenital flexion deformity at proximal interphalangeal joints of little finger is known as Camptodactyly. Dupuytren’s contracture, congenital absence of the extensor mechanism, a trigger finger and boutonniere deformity are also fall under the flexion deformities of fingers. Hence, such congenital anatomical knowledge is very important to radiologists, physiotherapists and orthopedic surgeons to avoid complications during radiodiagnostic procedures or surgeries of flexor deformities of fingers. Accessory muscles or tendons in the hand may lead to confusion during surgical procedures which results in errors in both diagnosis and treatment. There are many studies describing the anatomical variations in the origin and insertion of lumbricals, Kurzumi M et al. revealed that the lumbrical muscles originated from the intermediate tendon of the deep layer of the flexor digitorum superficialis of the index finger. 13 In this study bipinnate first lumbrical arising from the radial side of FDS and FDP tendons of index finger was noted. Such anatomical variations may interfere or disturb the biomechanics of FDS. Moreover, presence of hypertrophied lumbricals noted in this study can cause compression of the radial and ulnar digital arteries leading to chronic ischemia, hence a complete knowledge of lumbricals is essential during various surgical procedures of hand.
CONCLUSION As per review of literature combination of multiple anatomical variation of lumbricals in and around the carpal tunnel noted in this study, have not been reported in the literature till date. Awareness of these variations is necessary to avoid complications during radiodiagnostic procedures or surgeries in the antebrachial and hand during various surgical procedures.
REFERENCES
Policy for Articles with Open Access
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.