 Home
Home
|
Table of Content - Volume 21 Issue 1 - January 2022
A study on morphology of retro hepatic segment of inferior vena cava in Jharkhand population
Keshav Krishna
Tutor, Department of Anatomy, Phulo Jhano Medical College, Dumka, Jharkhand, INDIA. Email: keshavkrishna234@gmail.com
Abstract Background: Knowledge regarding morphology of Retro Hepatic segment of Inferior Vena Cava (RIVC) is important while performing procedures/surgeries on liver such as, hepatic vein catheterisation, selective venography, partial hepatic resection, liver transplantation. There is paucity of literature concerning morphology of RIVC in Jharkhand population. Thus, considering the applied importance of morphology of retro hepatic segment of Inferior Vena Cava (IVC), the present study was undertaken to describe the gross anatomy of RIVC. Aim and Objectives: To elucidate the variations in morphology and morphometry of cadaveric retro hepatic segment of inferior vena cava viz. its length and hepatic venous tributaries and its ostia in the population of Jharkhand, India. Material and Methods: The present work was carried out in the Department of Anatomy, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand. The work was carried out over a period of about one and a half year on ten embalmed adult cadavers during routine dissection in the dissection hall. Employing standard procedures retroperitoneal structures were dissected to expose IVC. Liver was dissected out along with the retro hepatic segment of IVC, posterior wall of RIVC was slit open and hepatic venous ostia were studied and measurements taken. Results and Discussion: - Length of retro hepatic segment (RHS) ranged from 4 cm to 7.8 cm. The average length of retro hepatic segment was 6.49 cm. Number of Hepatic venous ostia were two in 50% of specimens and three in rest 50%. Conclusion: The present study, conducted at RIMS, Ranchi, Jharkhand, gives knowledge about morphology of Retro Hepatic IVC in Jharkhand state. Results of this study will help clinicians for planning and executing surgeries and interventions on liver, and for routine classroom/dissection hall discussion. Key Words: Retro Hepatic Inferior Vena Cava, Morphology
INTRODUCTION The retro-hepatic segment of Inferior Vena Cava (IVC) occupies a deep groove on the posterior surface of liver or sometimes a tunnel completed by band of liver tissue, between the caudate lobe and right lobe of liver.3,4, 5 A long segment of IVC is resected during hepatic transplantation. Hepatic veins are important for circulation of blood through liver. These veins are catheterised with balloons to measure the pressure in the vein and the sinusoids, as in portal hypertension. Hepatic veins opening into IVC are called the ostia venae hepaticae, through which catheters are introduced into the hepatic veins [1]. Thus, considering the applied importance of the morphology of RIVC the present study was conducted. The hepatic veins drain blood from the liver into the Inferior vena cava. The tributaries arise within the parenchyma of the liver. The hepatic veins are arranged as upper (superior) and lower (inferior) groups. The superior groups are larger in size and commonly referred to as the right, middle, and left hepatic veins. Right hepatic vein drains segments V, VI, VII, and VIII. Middle hepatic vein drains segments IV, V and VIII. Left hepatic vein drains segments II, and III. The middle hepatic vein drains into Inferior vena cava separately or more commonly joins the left hepatic vein to form a short trunk. The lower group vary in number and are small veins draining directly into IVC from segment –I and occasionally from segment VII and VIII. The caudate lobe has small veins draining directly into the Inferior vena cava.1,2,4,5, 6 AIM AND OBJECTIVES: To elucidate the variations in morphology and morphometry of cadaveric retro hepatic segment of inferior vena cava viz. its length and hepatic venous tributaries and the number of hepatic venous ostia in the population of Jharkhand, India.
MATERIAL AND METHODS The present work was carried out in the Department of Anatomy, Rajendra Institute of Medical Sciences, Ranchi, Jharkhand. The work was carried out over a period of about one and a half year on ten embalmed adult cadavers during routine dissection in the dissection hall. Employing standard procedures Inferior Vena Cava was exposed with the help of scalpel, scissors and forceps. Retroperitoneal structures were dissected to expose IVC. Liver was dissected out along with the retro hepatic segment of IVC, posterior wall of RIVC was slit open and hepatic venous ostia were studied and measurements taken. Length was measured using string, divider, scale, measuring tape and slide calliper.
RESULTS Hepatic vein tributaries were studied by removing the liver along with the retro hepatic segment of the liver. The retro hepatic segment was not completely encircled by the liver tissue in any of the cadavers. The posterior wall of the retro hepatic segment of inferior vena cava was cut open and the hepatic venous ostia opening into IVC was studied. In the present study 25 large hepatic venous ostia were detected among the ten cadavers under study. It averages to about 2-3 large hepatic venous ostia in each cadaver. In five cadavers, three large hepatic venous ostia were seen draining into the inferior vena cava, while in the rest five only two large hepatic venous ostia were observed.
Table 1: Incidence of variation in number of hepatic veins
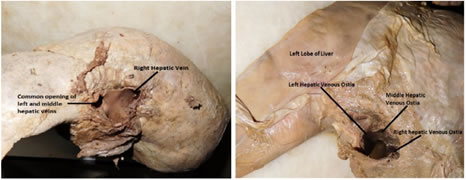
Figure 1 Figure 2 Figure 1: Two hepatic veins opening into IVC; Figure 2: Three separate Hepatic Venous Ostia opening in the Retro Hepatic segment of IVC
DISCUSSION Length of retro hepatic portion of IVC ranged from 4.0 cm to 7.8 cm with a mean value of 6.49 cm and S.D. of 1.36 cm [Table 1]. This is similar to various other such studies, where mean value ranges from 6.7 cm to 7.1 cm [Table 2].
Table 2: Comparison of length- Retro Hepatic Segment of IVC
Large size hepatic veins, which were clearly visible to the naked eye were studied. In five i.e., 50% cadavers three hepatic veins drained separately into inferior vena cava, while in the rest five i.e., 50% the middle and left hepatic veins drained through a common ostium, which is a deviation from the reported literature for combined ostia of LHV+MHV [Table 3]. This might be due to smaller sample size. The incidence of right hepatic veins draining separately into IVC in the reported literatures has varied from 83% to 100% [Table 3] which is comparable to the present study. The incidence of common ostia draining left and middle hepatic vein in various literatures has varied from 70% to 88% [Table 3]. Table 3: Comparison of variation in number of hepatic venous ostia
On an averages 2-3 large hepatic venous ostia were seen in each cadaver. This is comparable with other such studies. Ghosh et al. described median number of 7, range of 5-9.11 Change et al. reported mean number as 8.3,8 while Camargo et al. reported a mean value of 14.7 per liver. These higher numbers may be due to inclusion of both large and small sized hepatic venous ostia. The usual hepatic venous drainage has a specific pattern. Right hepatic vein drains segment V, VI, VII and VIII of liver. Middle hepatic vein drains segments IV, V and VIII. Left hepatic vein drains segments II and III of liver. These days liver transplantations are being carried out frequently. A sound knowledge of the morphology and drainage pattern of hepatic veins is essential for such procedures.
CONCLUSION This study will throw light on the morphology of retro hepatic segment of the Inferior Vena Cava, its tributaries, the hepatic veins and hepatic venous ostia in the local population of Jharkhand. This will help the clinicians and surgeons in planning and executing various interventions such as hepatic vein catheterisation, partial resection of liver and hepatic transplantations. It will also help in routine class room/dissection hall discussions and teaching.
REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.