 Home
Home
|
Table of Content - Volume 22 Issue 1 - April 2022
Anatomical variations of lateral femoral cutaneous nerve of thigh - A cadaveric study
J Jayarani
Professor, Department of Anatomy, Government Thoothukudi Medical College, Thoothukudi, Tamil Nadu, INDIA. Email: drjjanat2007@gmail.com
Abstract Background and Aim: Meralgia Paraesthetica is a neurological condition presented with burning sensation or numbness on the lateral aspect of thigh due to entrapment of Lateral femoral cutaneous nerve occurs during many surgical procedures like inguinal hernia repair, spine surgery and hip joint surgery. Knowledge about lateral femoral cutaneous nerve is very useful for various surgeons to improve their skills and success in their surgical procedures by avoiding surgical complications. Materials and Methods: 25 formalin embalmed cadavers were utilized for this study. By transperitoneal approach, lateral femoral cutaneous nerve, a branch of lumbar plexus was identified on both sides and it’s anatomical variations were tabulated. Results: High form of variations shows that, the LFCN arose from first and second lumbar spinal nerve in one cadaveric specimen and from second lumbar spinal nerve alone, in two cadaveric specimens. In the low form of variations, LFCN arose from third lumbar spinal nerve, seen in five cadaveric specimens, shows that this was the common form of anatomical variations of LFCN. In one cadaveric specimen, LFCN presented as a two branch arose from second lumbar spinal nerve and as a branch of femoral nerve respectively. Conclusion: Present study on formation and branching pattern of LFCN helps the clinicians to gain knowledge for clinical diagnosis of referred pain in the case of pelvic inflammatory disease and psoas abcess and for clinical procedures like lateral femoral cutaneous nerve block and lateral femoral cutaneous nerve graft. Keywords: low form, high form, meralgia paraesthetica, L-lumbar, LFCN.
INTRODUCTION Lateral femoral cutaneous is one of the lateral branches of lumbar plexus (Cunningham’s Manual of Practical Anatomy 16th edition Volume 1(168).It arises from the dorsal division of second lumbar spinal nerve and third lumbar spinal nerve and emerges from the lateral border of psoas major muscle and crosses the iliacus muscle obliquely towards anterior iliac spine after passing behind or through the inguinal ligament, medial to anterior superior iliac spine at a variable distance of 10 to 15 cm and divide into anterior and posterior branches, thereby enters the front of thigh, supplies sensory innervation to anterolateral aspects of thigh. (Gray’s anatomy, 41st edition 2016;(1371). Knowledge about anatomical variations of Lateral femoral cutaneous nerve is very useful for surgeons of various fields, to prevent it’s damage during many surgical procedures like, iliac crest bone graft and hip fracture surgery (Chinese journal of Primary medicine and Pharmacy;(12):1338 – 13421,2017)by orthopaedic surgeon, laparoscopic herniorrhaphy by laparoscopic surgeon, abdominoplasty by plastic surgeon ,spine surgery by neurosurgeon ,thereby avoiding the development of clinical condition known as Meralgia paraesthetica. Meralgia paraesthetica also known as Bernhardt – Roth syndrome, is neurological condition characterized by aching, stabbing, burning sensation or numbness in the lateral side of thigh occurs due to compression or damage to the lateral femoral cutaneous nerve of thigh. (JReconstr Microsurg 2006;22(5): 343 -348) Clinicians applying their anatomy knowledge of LFCN in diagnosing many clinical conditions like referred pain in pelvic inflammatory disease,Psoas abcess, sciatica and hip joint disease. AIM: Aimed to study the lateral femoral cutaneous nerve of thigh and it’s variations in relation to formation and branching pattern.
MATERIALS AND METHODS In this study, 25 embalmed cadavers received at Government Thoothukudi Medical College during different period of time, for first medical professional’s study purpose were utilized from March 2019 to December 2020. By routine transperitoneal approach lumbar plexus was explored on both sides, formation of lateral cutaneous was identified and traced from the lateral border of psoas muscle on either side. Variations in the branching pattern was noted and tabulated (Table 1). Routine dissection Instruments were utilized for this study.
RESULTS LFCN arose from L1 and L2 (high form) in 2% of specimens (Sim and Webb) and from L2 alone (high form) in 4% of specimens (De Ridder et al.). In 10 % of specimens , the LFCN arose from L3 alone (low form) (Hollinshed and Griffins) 2% specimens showed that ,the LFCN arose as a two branch from L2 alone (Anat Sci Int 2002 Dec 77(4);247-9,Variations of LFCN Erbill KM et al.). LFCN as a branch of femoral nerve was observed in 2% of specimens (Ronald A.Bergman ).40 % of specimens of our study presented with normal form of LFCN arose from L2 and L3 spinal nerves (J.Symington).
Table 1: Observation of variations in the formation of Lateral femoral cutaneous nerve of thigh.
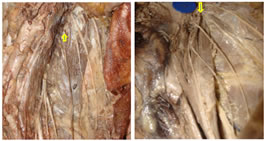
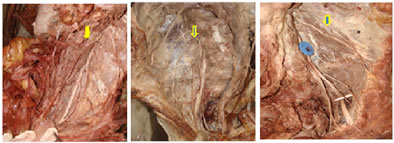
Figure 1 Figure 2 Figure 3 Figure 4 Figure 5 Figure 1: Lateral femoral cutaneous nerve from L1, L2-High form; Figure 2: Lateral femoral cutaneous nerve from L2 – High form; Figure 3: Lateral femoral cutaneous nerve from L3 – Low form; Figure 4: Lateral femoral cutaneous nerve as two branch; Figure 5: Lateral femoral cutaneous never as branch of femoral nerve
DISCUSSION Present study showed that, high form of variation of LFCN arose from L1,L2 was seen in 2% of specimens coincided with Deepti Arora et al. (1.67%), Sim and Webb reported (36.7%), De Ridder et al., found in 6% of specimens. In this study, LFCN arose from L2 alone (high form) was observed in 4% of specimens as compared to 1.7% in Sim and Webb study, 2.9% in Low form of LFCN from L3 alone was seen in 10% of specimen in our study while De Ridder et al. found in 6%. 2% of specimens in our study revealed that, the LFCN formed as two branches, presented like 3.5% of Erbill et al. study, as compared to 23% of Rosenberger, Loeweneck and Meyer study which was not coincided with our study. In the present work,2% of specimen showed that the LFCN arose from branch of femoral nerve similar to Ronald A.Bergmann, Diaz Filho (2003 ) and Denizuzmansel (2006) study showed 2% ,as compared to 10% in Sim and Webb and Anandhi et al. (10 %) (2018)(Table2). 80% specimens presented with normal form of LFCN, arose from L2 and L3 spinal nerves, coincided with J.Symnigton (1915).
Table 2: Comparison of present study with other authors (Philip A. Anloague ,et al.,)
CONCLUSION The current study concluded that, the variations in the formation of lateral femoral cutaneous nerve of thigh presented as high form in 6% of specimens and low form in 10% of specimens illustrated that the high form of variations were more common than other form of presentation. Thus, the knowledge of lateral femoral cutaneous nerve and its variations are very useful for general surgeons, plastic surgeon, orthopaedic surgeon while doing inguinal hernia repair, abdominoplasty and hip fracture surgery respectively to avoid injury to it, thereby preventing the development of neurological condition known as meralgia parasthetica. Many clinicians applying the knowledge of LFCN on clinical diagnosis of referred pain in the case of psoas abscess, pelvic inflammatory disease and sciatica, and also utilizing for management like lateral femoral cutaneous nerve block and lateral femoral cutaneous nerve graft in hip fracture surgery and facial nerve reconstruction surgery respectively.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.