 Home
Home|
Table of Content Volume 4 Issue 2 -November 2017
Variations in the shapes of the coronoid process of adult human mandible in Marathwada and Western Maharashtra region
Dhanaji S Jadhav1, Shashank B Vedpathak2*
1,2Associate Professor, Department of Anatomy, MIMER Medical College, Talegaon Dabhade, Pune-410507, Maharashtra, INDIA.
Abstract Background: Mandible is the strongest and largest bone of skull, having various morphological features which can be useful in identification of race, sex and age of the skeleton. Coronoid process can be an excellent graft for maxillofacial reconstructive surgeries. Aim: Primary aim of the present study is to find out various forms of coronoid process in Maharashtrian population and to discuss numerous factors responsible for it. Material and Methods: The study includes 130 mandibles (Male 82 and females 48) obtained from Department of Anatomy Government Medical College, Ambajogai, Government medical college, Solapur and Government Medical College, Nanded. Results and Conclusion: Triangular shaped coronoid process was found to be most predominant type (60.76%) followed by Hook (23.84%) and rounded (15.38%) types. Triangular shaped coronoid process was found to be significantly higher in females. Key Words: Coronoid process, triangular, hook shape and rounded shape.
Morphological variations are produced by the corresponding developmental variations through hereditary determinants and the functional changes, this takes place during the growth process. The muscle and bone may dynamically affect the function of each other and lead to the changes in the morphology of the bone involved.1 The mandible is the largest and strongest bone in the face. It has a horizontally curved body that is convex forward and two broad rami that ascend posteriorly. The rami bear the coronoid and condyloid processes. The coronoid process projects upwards and slightly forward as a triangular plate of bone. Its posterior border bounds the mandibular incisure, and its anterior border continues into that of ramus.2 For maxillofacial surgeons, Coronoid process among the two processes is very useful clinically can be used as graft for various surgeries. Its clinical application is also favourable because its size and morphology fits into the paranasal region, with the additional advantage of biocompatibility, availability and reduced operation time for harvesting.3 Previous scientists used various descriptive terms for coronoid process. The coronoid processes, coronoid means crow has been described as one of the bony processes of the ramus of the mandible.4T riangular process has been illustrated by Hamilton5, Romanes6, Snell7, and Basmajian8 et al. Schafer et al described the coronoid process as beak shaped.9 Presence of double or second coronoid process was also documented by Kansu H.10 Hence the present study was carried out to document different forms of coronoid processes of adult mandible in the regions of Maharashtra and to assess utility of this knowledge in identification of sex and race.
MATERIALS AND METHODS All the bones were collected from Departments of Anatomy of Medical Colleges of Ambajogai, Solapur and Nanded. A total of 130 mandibles i.e.82 males and 48 females were selected for the study. Unossified, deformed, fractured and decayed bones were excluded from the study. The various morphological forms of coronoid process were observed, documented and classified as follows. Triangular: apex is pointed straight upwards with straight anterior and posterior border. Rounded: apex is blunt, straight anterior and posterior border. Hook shaped: tip was pointing in backward direction with convex anterior and convex posterior border. The collected bones were analysed, for above different shapes and photographs were taken and findings were documented.
Figure 1: Triangular shaped coronoid process; Figure 2: Rounded shaped coronoid process; Figure 3: Hook shaped coronoid process OBSERVATIONS AND RESULTS Table 1: Various shapes of coronoid process
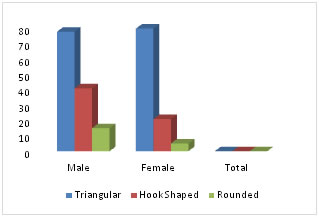
Figure 4: Graphical presentation of several types of coronoid process Overall triangular type of coronoid process (60.76%) is more prevalent than rounded (15.38%) and hook shaped (23.84%). Over all triangular type is more prevalent in males. In the following table, we compare our finding with the previous studies. Table 2: Comparison of numerous studies of coronoid process of mandible
From the above table, it becomes very much clear that nearly all populations show same pattern of diversity i.e. triangular shaped is most common followed by hook shaped then by rounded shaped. But the findings of Priyank Bhabhor (2015)18 was much different, as according to him hook shaped pattern of coronoid process is more common than triangular type. Clauser (1995)20 et al reported the use of temporalis myofascial flap both as a single and a composite flap with cranial bone, as the arteries supplying the coronoid process, arise from vessels that supply the muscles attaching to these processes, and generally not from the inferior alveolar artery which primarily supplies mandibular body and teeth.20 Information regarding the morphological shapes of the coronoid process is useful for the maxillofacial surgeon. The coronoid process can be used as an excellent donor graft site for reconstruction of orbital floor deformities. (MINTZ et al.,1998).21 CONCLUSION
REFERENCES
|
|

 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.