 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 1 -April 2019
Reasons of cancellation of elective cases on the day of surgery - A retrospective study
Assistant Professor, Department of Anaesthesia, MIMER Medical College, Talegaon Dabhade, Pune, Maharashtra, INDIA. Formerly as Freelancer Consultant Anaesthesiologist, PCMC Area, Pune, Maharashtra, INDIA. Email: shobhavatkar@gmail.com
Abstract Background and Aim: Hospitals invest major resources in maintaining and arranging Operation rooms, appointing anaesthetists, Operating surgeons, and OT staff to run an institute. But unindicted cancellation or postponement of operation is a major concern for an institute. On the day cancellation of proposed surgery is a major concern for inefficient use of Operation Theatre and waste of resources. Material and Method: This was a retrospective study of OT bookings (OT list) and IPD case papers of patients, posted for surgical cause; for consecutive five calendar years in various hospitals of PCMC area, Pune with notification of reasons for postponement. Cancellation of surgery is defined as any operation which is scheduled in OT list on Prior day by 3.00pm and is not performed on next intended day. Results: Out of 4500 patients, 85 (1.88%) patients were postponed on that day of surgery. The most common category was miscellaneous related 39 (45.88%), followed by medical 26 (30.59%), administrative 19 (22.35%) and patient related 1(1.176%). Conclusion: Elective cases postponement can be reduced by correct planning, Optimizing patients with pre anaesthesia OPD, Physician’s opinion and review, Discussing with nursing staff in advance and Communication with concerned anaesthesiologist. By appreciation of causes of case postponement on the day of surgery; can improve proper utilization of operation floor and OT suits by clinicians and administrators. While anticipating those patients in which problem may arise, essential attention can be paid in advance. Key Word: Operation rooms, Postponement, Surgery
INTRODUCTION Hospitals invest major resources in maintaining and arranging Operation rooms, appointing anaesthetists, Operating surgeons, and OT staff to run an institute. But unindicted cancellation or postponement of operation is a major concern for an institute for inefficient management and waste of resources. In recovery patients keep waiting for their turn and come mentally prepared, making all official and financial arrangements. But sometimes late postponement of operations is stressful from patient’s point of view for a productive population1. This results in wasted investigations and blood cross matching, and potentially affect patients’ outcome. This seems to be one of the quality indicators for an institute. By knowing the reasons, appropriate steps can be taken to reduce the rate to minimum. This is the retrospective study after seeing OT bookings and the IPD Indoor patients’ case sheet, for the reasons of postponement of elective cases, on that day of surgery; for consecutive five calendar years in various hospital of PCMC area, Pune, Maharashtra, India with an aim to find out the reasons of postponement for scheduled cases in OT list and to analyse the causes for optimum rectification.
MATERIAL AND METHOD The present study has been carried out by studying IPD sheets within five consecutive calendar years in various hospitals of PCMC, Pune area for all patients including major, minor and super-major cases. These patients were evaluated in Pre-anaesthetic OPD near recovery before posting them for surgery. Patients with co-morbid diseases need to optimise with treating physicians beforehand. Patients with Difficult intubation and Airway problems were intimated to concerned anaesthetists for better plan with ready difficult intubation trolley. Patients with prior Respiratory, Cardiac and Cerebrovascular diseases need to be evaluated further after correction. Lab was seen with accuracy. Geriatric patients were seen in their wards and with care due to associated problems. Patients in ICUs were evaluated with senior anaesthesiologists for expert’s opinion. A postponement of OT is defined as any operation which is scheduled in OT list on Prior day by 3.00pm and is not performed on next intended day. The reasons for postponement were noted by concerned Doctors and in-charge sister in a register with reason. Inclusion criteria
Exclusion criteria:
Statistical Analysis: Statistical analysis was done using MS OFFICE Excel version 5/95 software to calculate the percentage and drawing figures.
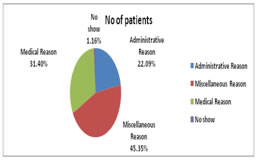
OBSERVATIONS AND RESULTS 4500 patients were posted for elective operations during study period .Out of these 2700 patients were male and rest 1800 were females. Out of 4500 patients, 85 i.e. (1.88%) patients were postponed on that day of surgery. 19 patients i.e.(22.35 %)were cancelled due reimbursement not approved. 26 out of 85 patients i.e. (30,58%) were cancelled due to medical reasons, 36 out of 85 i.e.(42.35%)were cancelled due to surgeons decision. 6 out of 85 i.e.(7.06%) got postponed in anaesthesiologist’s review. 1 out of 85 i.e.(1.17%)had no show , and 8 out of 85 i.e.(9.41%)patients were not willing for operation. 1 patient out of 85 i.e. (1.17%) got postponed due to surgeons delay to start and 15 out of 85 i.e. (17.64%) were posted in OT list though they were unfit. The reasons for cancellation are shown in Table 1. And percentage is shown in figure 1The reasons for cancellation were grouped as:
Table 1: Reasons for postponement
Figure 1 Administrative reasons
Miscellaneous reasons
Medical Reasons Were Two Types From surgeons side:
From Anaesthesia side:
Patient related reasons:
DISCUSSIONTo reduce the cost of surgery necessitates an efficient use of theatre time and personnel. The decision to postpone an operation in a scheduled list has psychological, social and economic impact. Though there is no acceptable rate of case cancellation, less than 5% is generally recommended. In the present study 1.88% of all scheduled surgeries were cancelled on the OT day during five consecutive calendar years in various hospitals in PCMC area, Pune, Maharashtra, India. This could have been potentially avoidable if planned properly. Schofield et al3 reported bed availability and theatre time management as a main reason for cancellation. In our study lack of available OT time was one of the reasons. Simple measures as room turnover time, Start of first case in time and setting up surgeons trolley and anaesthesia equipment save lot of time. Surgeon’s decision was the most common reason for cancellation in our study. Time taken for a particular surgery depends on skill and experience of operating surgeon. Less experienced and trainee surgeons take more time than expected. Sometime the time of surgery exceeds due to unanticipated complications and surgical findings during surgery. Technical issue may be faced due to unavailability of equipment’s. There was no record of estimated schedule time, and actual time taken by the surgeons. A study by Pandit JJ, Carry A4. Estimated that over-booking of operation list is the common cause for postponement due to waiting list pressures. This can be minimized by taking surgeon, anaesthesia, patient and OT staff into account while preparing the OT list. Windokun et al5 reported surgeon’s un-availability as main reason. Operation list is prepared by junior surgeon, after consultation with senior surgeons. In this study 8 cases were cancelled due to senior surgeons being not available due to either they were busy elsewhere in emergency operation, or were in important meeting, or due to ill health. A good communication between surgical team could have avoided such cancellation. Vinukondaiah6 cited fitness as main issue with many emergency surgeries during elective hours as main reason for postponement. Cancellation on medical ground were reported in 26 (31.40%) in our study. Good pre-operative assessment and timely correction by physicians could have avoided it. In this study, on table hypertension where hypotensive anaesthesia was expected, increased INR, physician’s opinion to withhold surgery till proper optimization, fever on the day of surgery, excessive VBPs on table, ST and T wave changes in ECG monitor were some of the medical reasons. Dufek7 et al recommended the improvement in protocol for pre-op patients’ evaluation to address these problems. Delay in laboratory reports were issues in 2 patients. Jonnalagadda et al [8] by statically correlated reasons by postponement as insufficient available beds, improper patient’s preparation, no show, and insufficient staff. Administrative related reasons accounted for 19(22.35%) of all cancellation in our study. Shortage of linen/equipment was the most common reasons. This happened due to poor communication and interdepartmental coordination. It should be noted as adverse event for the hospital. Patient related cancellation can be avoided by better communication between patient and surgical team to improve relationship. Two patients were cancelled in our study for not Nil by Mouth. Fasting guidelines should better be explained to patients and their relatives a day prior with reasons to avoid full stomach on operative day.To reduce the number of cancellation, recommendations could be by
CONCLUSIONPunctual OT staff, Meticulous planning, Keeping instruments/ drugs/ other equipment ready, Discussing plan of surgery with anaesthesia team, Getting assurance from OT staff, Discharging PACU (Post Anaesthesia Care Unit) patients promptly, Counselling patients efficiently and Provision of regular monthly audits are some of the measures, if timely rectified; can potentially avoid approximately 75% of cancellation of elective cases on the day of surgery.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.