 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 3 -June2019
A comparative study of analgesic efficacy of fentanyl and butorphanol for adult tonsillectomies under general anesthesia
B Vinod Kumar1, Shilpa Gaikwad2*, Jyotsna Paranjpe3
1,2Associate Professor, 3Junior Resident III, Department of Anesthesiology, BVUMC (Deemed to be University), Sangli, Maharashtra, INDIA. Email: docvinodreddy@gmail.com
Abstract Background: Relief of perioperative pain is a major concern for anaesthesiologists, surgeons, patient and relatives. Post-tonsillectomy pain is attributed to a combination of nervous irritation, inflammation, and spasm of the pharyngeal muscles. Acute postoperative pain after tonsillectomy surgery is an important factor as it causes many complications which can lead to morbidity, sometimes mortality also. Various analgesic drugs are in use for post tonsillectomy surgery and we plan to study fentanyl and butorphanol as analgesic for tonsillectomy Aims and Objectives: To evaluate and compare efficacy of intravenous fentanyl and intravenous butorphanol intraoperative, and postoperative analgesia in tonsillectomy surgery Materials and Methods: This study was done at Tertiary care hospital. ASA-I or II patients between 18-30 years of age, scheduled for Tonsillectomy surgery were randomly divided in two groups of 30 each. The patients receiving inj. Fentanyl(2mcg/kg) included in group A while-patients receiving inj. Butorphanol(40mcg/kg) included in group B for elective tonsillectomy under GA at time of induction for study purpose. Parameters recorded were Visual Analogue Scale(VAS), Pulse rate, Mean arterial pressure, Spo2, duration of surgery, duration of analgesia, need for rescue analgesia and complications Statistical analysis was done by using SSEP 22 version. Results: Data so collected was statistically interpreted. During postoperative follow-up intervals Butorphanol showed little longer duration of analgesia but there was no difference in VAS scores compared to Fentanyl. 4 patients from butorphanol group and 2 patients from fentanyl group complained of nausea. Conclusion: Compared to fentanyl, butorphaol is more effective for post-operative analgesic in terms of duration in patients undergoing for tonsillectomy surgeries Key Word: Analgesia, Butorphanol, Fentanyl, Pain, Tonsillectomy, VAS score
INTRODUCTION Pain has been defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage” (International Association forthe Study of Pain (IASP) 1986). Post-tonsillectomy pain is attributed to a combination of nervous irritation, inflammation, and spasm of the pharyngeal muscles. Acute post operative pain after tonsillectomy surgery is an important factor for post tonsillectomy Bleed which can lead to morbidity, sometimes mortality also. As pain increase patient hemodynamics may alter, irritability, nausea and vomiting hemorrhage, aspiration may occur Various analgesic drugs are in use for post tonsillectomy surgery and we plan to study fentanyl and butorphanol as analgesic for tonsillectomy Fentanyl Citrate Injection, is a potent opioid agonist. Fentanyl interacts predominately with the opioid mu-receptor but also binds to kappa and delta-type opioid receptors. These mu-binding sites are discretely distributed in the human brain, spinal cord, and other tissues. The principal actions of therapeutic value are analgesia and sedation. It has a rapid onset and effects generally last less than an hour or two. The analgesic effect of fentanyl is likely due to its metabolite morphine, which induces opening of G-protein-coupled inwardly rectifying potassium (GIRK) channels and blocks the opening of N-type voltage-gated calcium channels, thereby resulting in hyperpolarization and reduced neuronal excitability Butorphanol is a morphinan-type synthetic agonist–antagonist opioid analgesic. Butorphanol blocks pain impulses at specific sites in the brain and spinal cord. The exact mechanism of action is unknown Butorphanolis a mixed agonist-antagonist that exerts antagonistic or partially antagonistic effects at mu opiate receptor sites, but is thought to exert its agonistic effects principally at the kappa and sigma opiate receptors The purpose of this study is to evaluate the efficacy of postoperative analgesia by butorphanol tartrate in comparison with fentanyl hydrochloride after tonsillectomy
MATERIAL AND METHODS After IEC approval all adult patients of ASA grade I and II admitted for elective Tonsillectomy surgeries with adequate starvation under GA included for the study. After thorough pre anesthetic checkup patient has been explained regarding procedure and after taking consent. After receiving the study subject in pre anesthesia room, the baseline parameters noted. The patients have been explained about VISUAL ANALOGUE SCALE. All the patients premedicated with injection ondensetron 4 mg iv, injection gycopyrolate 0.2 mg iv, injection midazolam 1mg iv, injection fentanyl 2 mcg /kg iv or injection butorphanol 40mcg/kg iv, and anesthesia induced with injection propofol 2mg/kg and injection vecuronium 0.08-0.1 mg/kg. After direct laryngoscopy and endotracheal intubation done with appropriately sized endotracheal tube, anesthesia was maintained with sevoflurane 0.5-1.5% along with oxygen and nitrous oxide in a ratio of 1:2. Inj vecuronium 0.1mg/kg repeated as it was required. Reversal of muscle relaxation was done with injection neostigmine 0.05 mg/kg and injection glycopyrolate 8mcg/kg. Intraoperative monitoring was done as per standard protocols. Vital parameters such as Heart rate, systolic blood pressure, diastolic blood pressure, mean arterial pressure SPO2 and VAS score was monitored at 0min, 5min,10min,15min,30min,1hr,2hr and 4hr, 6hr,8hr, 10hr noted. Duration of analgesia is calculated as the time gap between the first injection of drug and subsequent dose on demand by patient. Duration of surgery was also recorded. Rescue analgesic in the form of injection Tramadol 50 mg intravenously will be given if VAS score is > 3. All the patients observed in post anesthesia recovery room and later in high dependency ward as per institutional protocol. A questionnaire prepared was filled up as per response of patients and charts will be maintained. Group A: receiving drug fentanyl(2mcg/kg) will be included in group A Group B: receiving drug butorphanol(40mcg/kg) will be included in group B Exclusion Criteria
Statistical Analysis for sample collection: Minimum sample size
n=2(Zα+Zβ)2 ∙ σ 2 = 30 δ2 where α= 5%, power=80% Statistical analysis: The data was entered in microsoft excel data sheet and analysed using spss22 version software. Categorical data represented in form of frequencies and proportions. Chi-square test used to analyse qualitative data. Continuous data represented as mean standard deviation. Paired t-test wastest of significance for paired data. p-value<0.05 was considered significant. OBSERVATION AND RESULTS Table 1: Demographic data
Demographic data was comparable with respect to Age, Weight, ASA physical status, Gender status and duration of surgery in both groups Pain Assessment: Pain assessment was done by recording the intensity of pain in a fixed-intervals by using VAS and rescue analgesic drug was used injection tramadol 50mg. The mean VAS for fentanyl group was 91.47min and for butorphanol group was 101min with P value <0.05
Table 2: VAS scores at 1st hour and 2 nd hour
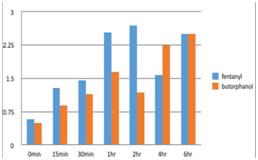
Graph 1: comparison of VAS scores in both the groups The graph is drawn VAS score against duration for fentanyl and butorphanol. RESULT There was no difference in VAS scores Table 3: Rescue analgesic time
Table 4: Complications
2 patients in fentanyl group and 4 patients from butorphanol group complained of nausea DISCUSSION The present study included and compared two opioids - butorphanol and fentanyl as choice of analgesic for tonsillectomy surgeries. Butorphanol is used to treat moderate to severe acute pain. Butorphanol injection was approved in 1978. it is agonist at kappa-receptor, but is a weak antagonist at μ-receptor3. Several clinical studies with the injectable form of butorphanol have shown its effectiveness in relieving moderate-to-severe postoperative pain. Fentanyl was discovered in 1960 by paul jessen. It predominantly acts at Mu receptor 1 9, 10, 11Since the study used identical protocols, the result obtained were comparable, combine analysis of the trial was valid The aim of this study was to know the efficacy of butorphanol in comparison with fentanyl with regard to postoperative pain. The patient’s age, gender, weight, duration of surgery was statistically not significant in two groups. Therefore, the effect of age, gender, weight, and duration of surgery would be minimized. Many of the earlier studies have used varying doses of butorphanol (20 μg/kg-40 μg/kg) and fentanyl (1-3 μg/kg). The study shows that butorphanol provides a little longer duration of analgesia than fentanyl Pandit et al compared butorphanol 40 μg/kg with fentanyl 2 μg/kg and reported a higher incidence of pain in fentanyl group and more drowsiness in butorphanol group. 40% of patients in each group required anti-emetic therapy. Hammad Usmani compared the same doses of butorphanol and fentanyl, but the incidence of drowsiness was not significantly different in both groups6 In a study conducted by Wetchler, he compared Butorphanol 20 μg/kg, butorphanol 40 μg/kg, and fentanyl 2 μg/kg and concluded 20 μg/kg butorphanol and 2 μg/kg of fentanyl appears to be suitable to use as a pre-induction narcotic analgesic7. hereas Butorphanol 40 μg/kg appears to be unsuitable due to increased duration of nausea, dizziness, time to reach a score of 10 on APARS and discharge- ready status. Patients in Butorphanol group showed significant levels of sedation, for first half hour none of the patients had any episode of desaturation (SpO2 <95%) and did not require any further intervention. This is may be due to kappa agonist effect of butorphanol. Usmani et al found that incidence of drowsiness in fentanyl group was as comparable as in butorphanol group6. Ahire SS et al. study during the first 30 minute in the postoperative period, patients receiving butorphanol had not complained of any pain whereas mean VAS Score was 3.13 in patients receiving fentanyl. Seventeen out of 30 patients (56%) required rescue analgesia in group F while no one from group B required rescue analgesia in first half hour postoperative period and the VAS score was found to be lower in group B when compared with group F till 1 hour postoperatively2 Post-operative side effects were compared in both groups. In our study 4 patients in butorphanol group complained of nausea and 2 patients in fentanyl group. Findings of Pandit et al also demonstrated that nausea and vomiting were the most common side effects in 55% patients of butorphanol group and 61% in the Fentanyl group. Thus in the present study, results suggested that butorphanol is an acceptable alternative opioid to fentanyl for its use as an analgesic for tonsillectomy surgeries
CONCLUSION On the basis of present study both fentanyl and butorphanol were found to be safe and comparable as analgesic in patients posted for tonsillectomy surgeries though butorphanol showed better results for duration of analgesia but as such no difference in VAS scores
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.