 Home
Home
|
Table of Content - Volume 18 Issue 3 - June 2021
Anaesthetic management in neonatal omphalocele with PDA, ASD, PAH - A rare case report
Panse Neha A1, Adate Kavia2, Khondalay Priyanka3*
1Associate Professor, 2Professor, 3Post Graduate, Department of Anesthesiology, Smt. Kashibai Navale Medical College and Hospital, Pune, Maharashtra, INDIA. Email: pkpriyanka14@gmail.com
Abstract Background: Neonatal emergencies have always put forth a challenge to the attending anaesthetist. Omphalocele is one among several neonatal emergencies. Omphalocele is an abnormal defect of the anterior abdominal wall and is often associated with cardiac anomalies. In this report we present a case of omphalocele and co-existing PDA with bilateral shunt, moderate PAH and ASD with Left to Right shunt and focus on the anaesthetic concerns and challenges encountered. Keywords: Omphalocele, PDA, ASD, PAH.
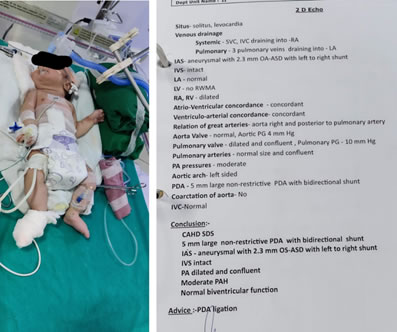
INTRODUCTION Omphalocele is one of the most common congenital anomaly of the anterior abdominal wall. It is a midline abdominal wall defect containing herniated viscera covered by a membrane. The outer surface of this membrane is known as amnion and the inner surface consists of peritoneum.1 It is often known to commonly occur in association with PDA and dextrocardia.2,3 There are several challenges encountered while handling these miniature ages. Underdeveloped systemic physiological functions, and their interactions with the anaesthetic agents present several difficulties. Our aim to report this case is to highlight the anaesthesia concerns and the challenges we faced while conducting this case. CASE REPORT PRE-OP A full term 1-day-old male child weighing 3.2 kg was admitted for repair of anterior abdominal wall defect [Figure 1]. The baby was born vaginally at 38 weeks of gestation with Apgar scores of 9 at both 1 and 5 min after birth. On physical examination the findings were, heart rate of 138 beats/min; blood pressure 70/52 mm Hg; SpO2 96% on oxygen hood with O2 at 2 litre/min; respiratory rate of 45 breaths/min; and temperature 36.5°C. Patient showed no apparent signs of respiratory distress on examination in supine position. Auscultation revealedclear lungs and precordium revealed pan systolic murmur on right side. Echocardiography detected a5mm large non- restrictive PDA with bidirectional shunt, IVS- intact, Moderate PAH, ASD with Left to Right shunt.[Figure 2]. USG abdomen pelvis showed the size of omphalocele defect as 7 cm. A peripheral intravenous (I.V.) cannula 24G was taken on right hand, and a maintenance infusion of Isolyte P with micro drip set at 2ml/kg (1 drip=16ml) was started. Prophylactic antibiotics were given according to baby’s weight. Preoperative laboratory results included a glucose level of 82 mg/dl and hemoglobin of 14.8 g%. The patient was posted for surgery on day 2 of life. Informed and written consent was taken from the parents and all associated risks and complications were explained including the need for postoperative ventilation. INTRA-OP In preparation for surgery, the room was warmed. Forced-air warmer was placed. On arrival ECG, (NIBP) noninvasive blood pressure and pulse oximetry were connected. Ringers lactate was started in the drip(1drip=16ml) for replacing intraoperative losses and as replacement for NBM hours. Preoxygenated and baby was premedicated with Inj glycopyrrolate, Inj midazolam and Inj Fentanyl according to weight. Patient was induced with Inj Propofol 6mg and Inj Atracurium 1.4mg IV. Trachea was secured with a 3.0-mm uncuffed endotracheal tube and maintained with 50% mixture of oxygen and air along with sevoflurane via Jackson Rees circuit. Caudal block was given in lateral position using Inj Bupivacaine 4.5ml 0.125%. After that patient was manually ventilated keeping all pressures within normal range. Nitrous oxide was avoided. An infant feeding tube was passed to suck out the gastric contents. On replacing the contents into the intraabdominal cavity a sudden fall in blood pressure (50/20 mm of hg) with tachycardia (190 / min) was noted. Patient was started on nor adrenaline infusion (0.05mcg/kg/min) which was continued 24 hours postoperatively and later weaned off. A rise in peak airway pressure was also noted which was <10 cm H2O along with hypotension and tachycardia. Primary closure could be achieved and the hypotension and tachycardia were managable. Inj Paracetamol 40mg was given after closure. The surgery lasted for 100 minutes. The baby was shifted to the Neonatal Intensive Care Unit (NICU) intubated where he was sedated and ventilated. POST-OP The baby was extubated 72 hours after the surgery. Orogastric feeding was resumed on the fourth postoperative day, and the baby was discharged on day 15 of life after ensuring adequate suckling efforts.
Figure 1 Figure 2
DISCUSSION Omphalocele and gastroschisis are the most common congenital anomalies of the anterior abdominal wall. Omphalocele has an incidence of 1 in 13000, whereas gastroschisis has an incidence of 1 in 5000–10,000. Up to 72% of neonates born with Omphalocele have associated anomalies and cardiac anomalies comprise 20% of these. Tetralogy of fallot and atrial septal defects are the most common cardiac anomalies associated withOmphalocele.4,5 These anomalies are routinely detected on antenatal ultrasound done along with anomaly scan to rule out associated congenital abnormalities. Babies with omphalocele need NICU admission for conservative management as well as pre and postoperative surgical observation. Management mainly emphases on fluid resuscitation, care of the herniated bowel and its blood supply, bowel decompression using a nasogastric tube, and temperature regulation. All blood investigations including complete blood count, renal function tests, liver function tests, chest X-ray, 2D Echocardiography should be done. In neonates with omphalocele ultrasound kidney pelvis, chromosomal analysis, and computed tomography head are performed to exclude the presence of other associated congenital anomalies. Cross-matched blood should be arranged for intraoperative transfusion if required. Care of the newborn with abdominal wall defects begins with preoperative assessment and optimization. After stabilization of the newborn, the exposed abdominal contents should be covered with a warm sterile moist dressing as was done in our case to prevent temperature and fluid loss from the herniated contents. These babies are prone to hypoglycemia; therefore, 10% dextrose 1-2ml/kg containing fluids should be given for maintenance and prevention of hypoglycemia. In our case the baby was started onisolyte -P. A Nasogastric tube was passed in our case to decompress the bowel and prevent regurgitation. Even if these babies are not fed, they should be considered as full stomach because of the inflammatory exudates in the bowel secondary to exposure to the amniotic fluid in utero. A patent I.V access should be ascertained in either upper limbs so that the venous return is not hampered post return of bowel after surgery. All such babies should receive appropriate antibiotics preoperatively to reduce the chances of intra-abdominal sepsis. Serum electrolytes should be tested, and electrolyte imbalances should be corrected before surgery. In our patient the electrolytes were within normal limits as per age. Due care must be taken during manipulation to avoid trauma to the abdomen and its contents. All neonates have a tendency for hypothermia due to increase body surface area more so in neonates with omphalocele because of the exposed bowel. Hence maintaining normothermia is encouraged by using warm incubator for shifting, ensuring theater temperature at least 27°C, using warmers to warm the mattress, covering the head to prevent loss of heat, using fluid warmers to infuse warm fluids, covering the exposed surgical site with moist warm dressings intraoperatively. Our patient was shifted in incubator and was completely covered with warming sheets except for surgical site. Fluid warmer was used and the operating room air conditioner was turned off.5 Difficult airway with large head, anterior placement of larynx, subglottic narrow area and poor oxygen reserves were taken care with pediatric Airtraq video laryngoscope, ETT no.3.0 and rapid sequence induction, which in turn also prevented the risk for aspiration which is very high in these tiny patients. Nitrous oxide was avoided during the maintenance due to its properties of causing distension of bowel which can increase intra-abdominal pressure on returning bowel contents to the abdomen during closure. An oxygen air mixture was used to maintain saturation around 90% as 100% oxygen can increase the risk of retinopathy in neonates. A special word of caution regarding anesthetic considerations of Patent ductus arteriosus with shunt. Measures were taken to prevent fall in peripheral vascular resistance and maintaining it above systemic vascular resistance, preventing reversal of shunt. Vasopressors were kept ready as per body weight for use in case of emergency. There are high chances of hypotension after returning herniated contents to the abdominal cavity due to decrease in pre load because of compression of inferior vena cava. One such episode was encountered in our case and was managed with vasopressor agents.6,7 Repositioning of the abdominal contents in the thoracic cavity may hamper Ventilation and respiration as it decreases pulmonary compliance and diaphragmatic excursion. Monitoring of peak airway pressures is a major concern following closure if the defect is more than 4 cm. In our case it was 7 cm and there was a transient rise in peak airway pressure which resolved after 30 minutes. A rise in the intra-abdominal pressure affects renal blood flow subsequently reducing urine output hence urine output should be judiciously recorded. Elective postoperative ventilation is the modality of choice to optimize the respiratory function compromised due to raised intra-abdominal pressure.
CONCLUSION Though presenting in emergency, thorough understanding of congenital cardiac anomalies, preoperative optimization, a vigilant intra and postoperative monitoring along with counselling for regular followups can improve the outcome by many folds in these tiny people.
REFERENCES
Policy for Articles with Open Access: Authors who publish with MedPulse International Journal of Pediatrics (Print ISSN: 2579-0897) (Online ISSN: 2636-4662) agree to the following terms: Authors retain copyright and grant the journal right of first publication with the work simultaneously licensed under a Creative Commons Attribution License that allows others to share the work with an acknowledgement of the work's authorship and initial publication in this journal. Authors are permitted and encouraged to post links to their work online (e.g., in institutional repositories or on their website) prior to and during the submission process, as it can lead to productive exchanges, as well as earlier and greater citation of published work.
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.