 Home
Home
|
Table of Content - Volume 19 Issue 2 - August 2021
Evaluation of efficacy and hemodynamic stability of propofol- ketamine and propofol-fentanyl in patients undergoing dilatation and curettage
Jinal Manek1, Kanchan Rupwate2*
1Assistant Professor, Department of Anaesthesiology, Grant Government Medical College and JJ Hospital, Mumbai, Maharashtra, INDIA. 2Additional Professor, Department of Anaesthesiology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, Maharashtra-400022, INDIA.
Abstract Background: To evaluate and compare the efficacy and hemodynamic stability of ketamine / fentanyl along with propofol and also assess recovery profile, post-operative analgesia and complications in patients undergoing Dilatation and Curettage (DandC). Method: Total 100 patients of ASA grade I and II, age between 18-55 years were enrolled and divided into two equal groups with adjuvant drugs in group PK- ketamine (0.75mg/kg IV) and in group PF-fentanyl (2ug/kg IV). Both groups received induction dose of Propofol- 2-2.5 mg/kg. Depth of sedation maintained with 0.5 mg/kg boluses of Inj.Propofol and assessed with Ramsay Sedation Score (RSS). The total dose of propofol was noted in both the groups. Intraoperative and postop vital parameters and complications were compared. Visual Analog Scale(VAS) was recorded and if VAS Score >6, then patients received Inj.Paracetamol 15mg/kg IV as rescue analgesia. The recovery was assessed by Modified Aldrete Score (MAS). The time from completion of procedure to reach MAS of 9-10 was noted. Results: The hemodynamics was better with ketamine than fentanyl group. The total dose of propofol requirement, intraoperative and postop complications, and VAS scores were higher in group PF than in group PK, thus more patients required rescue analgesia in fentanyl group as compared to ketamine group. The recovery was delayed in ketamine group as compared to fentanyl (higher MAS and prolonged time to reach MAS>9). Conclusion: Ketamine (0.75 mg/kg) provides better perioperative hemodynamic stability with good analgesia and fewer complications as compared to Fentanyl (2ug/kg) in patients undergoing DandC. Keywords: Propofol, Ketamine, Fentanyl, Sedation, Hemodynamic stability, Dilatation, Curettage
INTRODUCTION Dilatation and Curettage (DandC), is a short lasting but painful surgical procedure, performed for the diagnosis and treatment of endometrial and intrauterine disorders. It causes significant pain due to cervical dilatation with dilators and tissue extraction.1 Therefore, drugs that are used for this procedure, should ensure a rapid onset of action, an adequate level of sedation, good analgesia as well as rapid recovery. The most important objectives in the perioperative period being maintenance of the hemodynamic-respiratory stability and minimizing the side effects of the drug. Propofol is a widely used sedative agent due to its rapid onset of action and fast recovery time, but it causes cardiovascular and respiratory depression in a dose dependent manner. Also it might be insufficient in painful processes, if used alone since it lacks analgesic properties.1 Combining propofol with other drugs such as opioids or ketamine is recommended for improving the quality of sedation, analgesia and minimizing the potential adverse effects with maintainance of a stable cardiovascular and respiratory status in the perioperative period.2Ketamine, a NMDA receptor agonist, in subanesthetic doses with propofol has gained attention in total intravenous anesthesia because of its powerful analgesic action without causing myocardial and respiratory depression. Ketamine also causes some degree of sympathetic stimulation, which tends to counter balance the cardiovascular effects of propofol.3 Fentanyl on the other hand is synthetic opioid analgesic which has rapid onset and short duration of action and has been used in combination with propofol satisfactorily. The present observational study was carried out to assess and compare the clinical efficacy and hemodynamic stability, recovery profile and side effects, if any in patients undergoing dilatation and curettage (DandC) under short general anaesthesia (TIVA) using propofol-ketamine and propofol-fentanyl drug combination.
After obtaining Institutional Ethical Committee approval, this prospective observational study was conducted in Gynecology OT and Labour OT of a tertiary care hospital from November 2016 to August 2018. Total 100 female patients of ASA grade I/II, aged between 18 to 55 years in two groups of each of 50 patients, posted for DandC under general anaesthesia using inj.propofol-ketamine or propofol-fentanyl were enrolled. Patients with co-morbid conditions such as diabetes mellitus, hypertension, ischemic heart disease and renal, hepatic insufficiency or chronic pulmonary disease, chronic use of sedative or opioid analgesics or on beta blockers, presence of psychiatric disorders, patients having allergy to egg or fat and patients with difficult airway were excluded from the study. A complete pre-op assessment was carried out and all relevant investigations were done. The procedure and grading of pain was explained to the patients during pre-anesthetic visit. Written valid informed consent checked and ASA fasting guidelines followed. All patients in both the groups underwent routine standard protocol for the operation, which was followed in operation theatres of our institute. Monitors attached to the patient and baseline parameters such as HR, BP, SPO2, RR were noted. Securing peripheral I.V line on non-dominant hand was drawn and ringer Lactate solution @ 2ml/kg/hr was started. Inj. Glycopyrolate 0.2 mg. and Inj. Midazolam 1mg intravenously slowly and oxygen supplementation with Hudson mask @ 4-6litres/min was given. Group PK (50 patients) received Inj. Ketamine in dose of 0.75mg/kg body weight IV slowly while group PF (50 patients) received Inj. Fentanyl citrate in the dose of 2 ug/kg body wt. as slow intravenous injection. After 5 minutes, in both the groups Inj. Propofol was given in the induction dose of 2-2.5 mg/kg body weight, slowly at the rate of 1 ml/3 seconds till the loss of eyelash reflex. During intraoperative period, blood pressure (BP), heart rate (HR), respiratory rate (RR), and peripheral oxygen saturation (SPO2) were recorded at time intervals of every 5mins for 30 mins or till the procedure was completed, maximum upto 45 mins in both the groups. Depth of sedation was assessed with Ramsay Sedation Score (RSS) at 5 mins interval until the end of surgery. The patients RSS score was maintained at 4-5 with an additional 0.5 mg/kg of bolus dose of Inj. Propofol iv was given when the patient became light as indicated by rise in HR, BP, lacrimation or any movement to surgical stimuli. The total dose of propofol required for the procedure was noted in both the groups. During the procedure, complications and side effects such as hypotension, bradycardia, nausea, vomiting, respiratory obstruction, respiratory depression or apnea, bronchospasm, abnormal movements, were noted and corrective measures taken accordingly. If respiratory obstruction occurred, airway manipulations were done by using maneuvers like head tilt, cssshin lift, jaw thrust. If respiratory depression occured, then intermittent positive pressure ventilation with mask or endotracheal intubation was done. Patients were withdrawn from the study if the planned procedure was changed over to major surgery or required endotracheal intubation. If there was fall in MBP below 20% or lower than baseline, then Inj ephedrine 6mg IV was given. If there is fall in heart rate less than 20% of the baseline with hypotension then Inj. Atropine 0.6mg IV was given along with IV fluids. Postoperatively, all vital parameters and Visual Analog Scale (VAS) was recorded every 15 minutes till 2 hours in both the groups. If VAS Score >6 then patients were given Inj Paracetamol 15mg/kg IV as rescue analgesia. The recovery was assessed by Modified Aldrete Score (MAS) in the post anesthesia care unit (PACU). The time from the completion of the procedure to reach MAS of 9-10 was noted. Complications in postoperative period such as nausea, vomiting, desaturation, pain, hallucination, dysphoria were noted. Statistical Analysis Statistical analysis was performed using SPSS (statistical package of social sciences), P value <0.05 was considered significant. Continuous variables like age, weight, systolic blood pressure (SBP), diastolic blood pressure (DBP), mean blood pressure (MBP), RR, SPO2 were expressed as mean±SD. For categorical variables like ASA group distribution, Chi square test was used. Paired T test was applied within the group for hemodynamic parameters. Comparison among different groups with respect to hemodynamic parameters was done with Independent T-test. Comparison of VAS was done using Mann Whitney U Test. Ramsay Sedation Score and MAS were done using Wilcoxon sum rank test.
RESULTS There was no statistically significant difference found between two groups (p>0.05) with respect to demographic profile- age, weight and ASA grade. Hence both the groups were comparable as shown in table 1.
Table 1: Demographic Characteristics of Patients
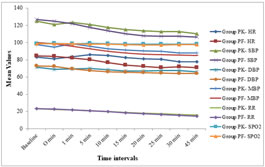
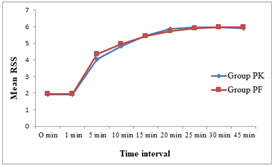
Figure 1 Figure 2 Figure 1: Comparison of intraoperative HR, SBP, DBP, MBP, RR and SPO2 between two groups; Figure 2: Comparison of Ramsay Sedation Score in both Groups Intraoperatively, there was fall in HR, SBP, DBP, MBP, RR, SPO2 which was statistically significant in group PF than group PK. (P value < 0.05) (Figure 1). However, postoperatively there was no difference between two groups in regards to hemodynamic parameters but difference in the fall in SPO2 of group PK and group PF was statistically significant after 30min (P<0.05). The Ramsay Sedation Score was higher in group PF than group PK at 5 min which was statistically significant, (P<0.05), (Figure 2). The total dose of propofol required in group PF was higher (113.8000±11.0915) than that in group PK (104.3878±15.4324), which was statistically significant, ( P = 0.001). VAS scores higher in group PF than PK group, the difference being statistically significant, (P<0.05), (Table 2). Thus more patients required rescue analgesia in fentanyl group as compared to ketamine group.
Table 2: Comparison of postoperative Visual Analog Scale in both groups
The difference in postoperative MAS in both the groups was statistically not significant, (P>0.05) except at 60 min. The recovery was delayed in ketamine group (MAS>9= 62.14±12.25 min) as compared to fentanyl (MAS>9= 60.9±8.7883 min) (higher MAS and prolonged time to reach MAS>9) but was statistically not significant. Intra and postoperative complications were significantly higher in group PF than in group PK as shown in table 3. In group PK, 2 (4%) patients required paracetamol as rescue analgesia as compared to group PF, where 6 (12%) patients required paracetamol as rescue analgesia. Table 3: Comparison of intra and postoperative complications between two groups
Nowadays, intravenous sedation techniques are widely used for DandC for good sedation, maintaining hemodynamic-respiratory stability and better analgesic management with minimal the side effects of drugs. Propofol, since its introduction in 1986 has been shown to have many of these properties. Many studies have been performed to assess propofol both as a sole anesthetic agent and in combination with fentanyl and ketamine in different dosages. However there are no studies about comparisons with the combinations of propofol along with either Fentanyl 2 microgram/kg or Ketamine 0.75 mg/kg for DandC under general anesthesia. Hence whether pre induction with ketamine 0.75 mg/kg or fentanyl 2 microgram/kg in combination with propofol as an inducing agent in a dose of 2-2.5 mg/kg for short surgical procedures like DandC offered any advantage in terms of better quality of anesthesia, hemodynamic stability, good recovery profile and minimal side effects was studied and compared to know the advantage of one combination over the other in the intraoperative and postoperative period. In the present study, perioperative heart rate was decreased significantly in group PF and this decrease in the HR can be attributed to the action of fentanyl on the cardiovascular system. Carotid sinus baro receptor reflex control of HR is markedly depressed by fentanyl causing dose dependent decrease in HR. Similar findings are reported in the previous studies2-5. The minimal fall in SBP, DBP and MBP in group PK as compared to group PF is due to the sympathomimetic activity of ketamine which counteracts with the cardiovascular depressant action of propofol, thus maintaining a stable hemodynamic profile as compared to fentanyl. These findings are correlated well with the study done by Pawar et al.4, Phillips et al.6 and Khutia et al.7. The opposing effect of ketamine and propofol on arterial pressure tended to cancel each other out resulting in improved cardiovascular stability.The propofol ketamine group experienced a smaller percentage decrease in SBP, which is comparable with other studies.2,3,8The reason could be as ketamine neutralized the cardiodepressant effect of propofol, there was better hemodynamic stability in group PK than in group PF. The fall in respiratory rate was higher in group PF than group PK due to respiratory depressant effect of fentanyl and preservation of airway reflexes and ventilation due to action of ketamine. Similar to the present study, in Pawar et al. study4 there was minimal change in respiratory rate during post induction and maintenance period. This is probably due to the lower dose of fentanyl (1.5ug/kg) used as compared to current study where fentanyl was given in the dose of 2ug/kg. However, Arikan et al. 2 found no significant difference in fall in SPO2 in both the group. This can be explained as remifentanil (1ug/kg) was used in this study as compared to fentanyl (2ug/kg) used in our study. There was no significant difference found in the RSS between PK and PF group, except at 5 mins, reason being administration of propofol 5 mins after the adjuvant drug was given. These results are comparable with the study done by Akhondzadeh.5The mean total dose of propofol required in group PF (113.8000±11.0915mg) was higher than that in group PK (104.3878±15.4324), which is correlated with the earlier studies.2,5,6 The VAS was statistically higher in group PF than in group PK. The analgesic property of ketamine could be attributed to the inhibitory action of ketamine at NMDA receptors which are important in pain processing and the modulation of pain. And hence, the requirement of rescue analgesia was lower in group PK than in group PF (P value<0.05). These findings are consistant with the previous studies.1,6,9 The recovery time in terms of MAS was prolonged in ketamine group as compared to fentanyl group but it was not statistically significant. Also time to reach MAS of >9 was statistically not significant in both the groups. (P value >0.05). these result are comparable with the other studties.2, 4, 7,10,11 The intraoperative complications were higher in group PF than in group PK. The ketamine–propofol combination is thought to act by counteracting the cardiovascular side-effects of each other, preserving the sedative efficacy. Also the amount of propofol needed to achieve a deep sedation level was much lower in case of PK group than PF group, which contributed to the lower incidence of hypotension and apnea. Also, no patients in present study required airway manipulation. The post operative complications were also higher in group PF than in group PK. There were no incidences of psychedelic effects of ketamine like hallucination, dysphoria and psychotomimetic emergence reactions when ketamine is used in combination with a sedative-hypnotic (e.g., benzodiazepines, propofol) or a general anesthetic (e.g., halothane, nitrous oxide) is minimal or negligible. Hypnotic doses of propofol are reported to block these hallucinations. These findings are concordance with the study done by Arikan et al.,2 Brajesh et al.,3 Mahajan. et al.8CONCLUSIONA multidrug intravenous regimen consisting of Ketamine (0.75ug/kg) as an adjuvant compared to fentanyl (2 ug/kg) is more efficacious and provides better perioperative hemodynamic stability with good analgesia with less requirement of rescue drug in post operative period and fewer perioperative complications. We have not encountered any psychotomimetic effects of injection Ketamine in the 0.75mg/kg dose, this effect may be masked due to preinduction administration of Inj.Midazolam. Hence propofol-ketamine combination is a better choice especially when hemodynamic stability is of great importance in patients undergoing diltation and curettage.REFERENCES
Policy for Articles with Open Access
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.