 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 4 Issue 1 -October 2017
Pradeep1, Raveendra U S2*
1Senior Resident, Department of Anesthesiology, Gulbarga Institute of Medical Sciences, Gulbarga, Karnataka, INDIA. 2Professor, Department of Anesthesiology, K. S. Hegde Medical Academy, NITTE University, Mangalore, Karanataka, INDIA. Email: adee217@gmail.com
Abstract Background: Delayed recovery or emergence can occur after general anaesthesia and it is one of the major challenges for an anesthesiologist. The time to recovery from anesthesia is affected by patient factors, anesthetic drugs, duration of surgery, and presence or lack of painful stimulation. In our study we found a higher incidence of delayed recovery from anesthesia with the use of sub-anesthetic doses of ketamine (0.5mg/kg) given during induction of general anesthesia Aims and objectives: To evaluate the recovery characteristics with the use of subanaesthetic doses of ketamine during general anaesthesia Material and Methods: One twenty adult patients of age between 18 and 45 years and of ASA grade 1 and 2 of either sex who underwent elective surgery at K. S. Hegde Medical Academy were included in the study. Patients were divided randomly into two groups of 60 patients. Groups were (a) Group KF with ketamine (0.5mg), fentanyl (2µg/kg) and propofol (2mg/kg), (b) group FP with fentanyl (2µg/kg) and propofol (2mg/kg). Recovery was assessed by modified Aldrete’s scoring system immediately at the end of surgery, 30 minutes and 1 hour after surgery Results: there was delayed recovery in group KF immediately and 30 minutes after extubation, whereas there was complete recovery after 1h in both the groups. Conclusion: addition of even a sub anaesthetic dose of ketamine during induction of general anaesthesia results in delayed recovery, this is an interesting finding as the duration of action of ketamine is short and thus further investigation is needed to confirm these observations and also to understand the underlying mechanisms. Key Words: Recovery; Ketamine; Fentanly; Propofol; Modified Aldrete’s score.
Recovery phase is important phase of general anesthesia which is of great physiological stress. Patients cannot be considered fully recovered until they have returned to their preoperative physiological state. Recovery is progressive improvement in level of consciousness, return of protective reflexes and cognitive function. Delayed recovery is one of the major challenges for an anesthesiologist. Aetiology is multifactorial ranging from patient to surgical factors. Because of its inherent effects on CNS, ketamine could be blamed for delayed recovery from general anaesthesia1. Ketamine is a NMDA receptor antagonist, which acts by non-competitive blockage, binding itself to the intra-channel phencyclidinic site and changing the channel opening time. Ketamine affinity for this binding site is three to four times higher compared to isomer. Analgesic potency of ketamine is two times that of racemic mixture. When administered both prior to anesthesia induction and throughout the perioperative period, ketamine is able to promote significant reduction in the consumption of anesthetic agents during surgical anesthetic procedure, exerting an “opioid sparing” effect, aside from promoting adequate postoperative analgesia2,3. Ketamine binds noncompetitively to the phencyclidine binding site of NMDA receptors but also modifies them via allosteric mechanisms. When studied at subanesthetic doses, its analgesic efficacy correlates well with its inhibiting action on NMDA receptor-mediated pain facilitation and a decrease in activity of brain structures that respond to noxious stimuli4. Ketamine therefore represents a promising modality in several perioperative strategies to prevent pathologic pain. Another reason for the renewed interest in ketamine is the availability of ketamine. Ketamine has a chiral center at the carbon-2 atom of the cyclohexanone ring, and therefore exists as the optical stereoisomers and ketamine. Therefore in this study, we have evaluated the recovery and complications from general anesthesia following analgesic doses of ketamine administered during induction of general anesthesia.
MATERIALS AND METHODS This is a prospective double blinded randomized controlled study. Patients were randomized into two groups of 60 patients each - Group KF: ketamine (0.75mg/kg) and fentanyl (2µg/kg) and propofol (2mg/kg) and Group FP: fentanyl (2µg/kg) and propofol (2mg/kg). Patients aged between 18 to 45 years; belonging to American Society of Anesthesiologists (ASA) physical status I and II who were scheduled for elective surgery under general anesthesia were included in the study. We excluded patients with hypertension, pregnancy, anticipated difficult airway and contraindications to any of the drugs. Anesthetic technique: After securing intravenous (IV) line with 18G IV cannula, monitors were connected which include ECG, pulse oximetry and noninvasive BP. Baseline values were recorded. Patients in group KF, drugs were given in the following sequence by intravenous route: fentanyl 2.0 μg/kg, followed 2minutes later by ketamine 0.5 mg/kg and after further 2minutes by propofol 2.0mg/kg followed by Inj. Atracurium 0.5mg/kg. Patients in group FP, drugs were given in the following sequence by intravenous route: fentanyl 2μg/kg, followed after 2minutes by normal saline, after further 2minutes by propofol 2mg/kg followed by Inj. atracurium 0.5mg/kg. After ensuring the proper placement of endotracheal tube patient was connected to mechanical ventilator. Anesthesia was maintained with oxygen: nitrous oxide in 1:2 ratio and isoflurane 0.6- 1% and positive pressure ventilation. ETCO2 was maintained at30-35 mmHg. Muscle relaxation was maintained with Inj. atracurium top ups guided by TOF monitoring. At the end of surgery, after discontinuing isoflurane, neuromuscular blockade was reversed with Inj. neostigmine and Inj. Glycopyrrolate. Extubation was done after complete recovery and adequate reversal. Patient recovery was assessed by modified Aldrete’s scoring system, immediately after recovery, after 30mins and after 1 hour. RESULTS The patients in both the groups were similar in terms of age, body weight, ASA physical status and duration of surgery. Student T test was done to compare the Modified Aldrete’s score and individual parameters. Modified Aldrete's scores, both immediately and 30 minutes after recovery were lower in group KF and was statistically significant with a P value of <0.001. Modified Aldrete's score 1h after recovery is lower in group KF and was statistically not significant with a P value of 1 (Table 1)
Table 1: General demographic data of the patients
Table 2: Modified Aldrete's score after recovery of the patients
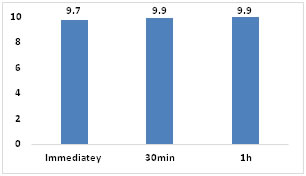
Figure 1: Modified Aldrete’s score – Group FP Figure 2: Modified Aldrete’s score – Group KF Figure 3: Parameters affected in Modified Aldrete’s score
Consciousness and circulation are the two parameters affected in Modified Aldrete’s score, in this study. Patients in group KF had decreased level of consciousness than FP. The difference is statistically significant immediately after recovery and at 30min after recovery, with a P value of less than 0.001 and the difference is not statistically significant after 1h with a P value of 0.159 Patients in group KF had higher blood pressure during recovery as observed by circulatory parameters in Modified Aldrete’s scoring system. The difference in circulatory parameter is statistically significant immediately after recovery with a P value of 0.001. Complications: One patient in group KF had an episode of bronchopasm following intubation, which was relieved after giving Inj. Deriphylline and Inj. Hydrocortisone 100 mg IV.
DISCUSSION Ketamine is a NMDA receptor antagonist with a short duration of action. In a previous study combination of ketamine and propofol provided adequate surgical conditions and better recovery profile when compared to fentanyl propofol combination3. In contrast, our study found delayed recovery when ketamine was added to fentanyl and propofol combination during induction of anesthesia. White et al.4 did a study to evaluate the brain and plasma concentrations of ketamine in rats after intramuscular injection of ketamine alone or intramuscular injection of ketamine with halothane anaesthesia. They found that the brain concentrations of ketamine after halothane anaesthesia were twice as high as those after ketamine alone. They concluded that the half-life of ketamine in plasma and brain is significantly prolonged by halothane anaesthesia. Thus further investigation is required to find out a possible synergistic interaction between ketamine and isoflurane, similar to that described for ketamine and halothane. There is a study that assesses the analgesic effect of ketamine-remifentanil combination5. Several studies of other surgical procedures were conducted using ketamine and remifentanil6-9. Due to the effects on NMDA receptors, ketamine can reduce central sensitization and intensity of postoperative pain. The combination of ketamine and remifentanil may promote prolonged analgesia, since this opioid’s great disadvantage of producing no analgesic effect after infusion discontinuation. A study has shown that ketamine administration both before induction of anesthesia and during surgery markedly reduced the need for opioids, in addition to adequate postoperative analgesia5. Pain therapy can be improved using intraoperative and postoperative ketamine in a variety of surgical procedures and anesthetic techniques. In particular, the intraoperative use of intravenous subanesthetic ketamine in general anesthesia provides pain prevention in the postoperative period10-12. The most important limitation to the available studies is the lack of evaluation of long-term outcome measures. We do not know whether ketamine use will translate into better recovery profiles or improved functional outcome.
CONCLUSION Addition of even a sub anesthetic dose of ketamine during induction of general anaesthesia results in delayed recovery. This is an interesting finding as the duration of action of ketamine is short and thus further investigation is needed to confirm these observations and also to understand the underlying mechanisms.
REFERENCES
|
|


 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.