 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 6 Issue 2 - May 2018
Original Research Article A comparative study of haemodynamic and electrolyte changes between 1.5% Glycine and distilled water as irrigation fluid for transurethral resection of prostate surgeries
Shilpa Gaikwad1, Jyotsna Paranjpe2*, Ravikiran Thote3, Prashant Lomate4, Sanjay Purohit5
{1Associate Professor, 2Professor, 3Sr. Resident, 4Assistant Professor, Department of Anaesthesia} {5Assistant Professor, Department of Uro Surgery} Bharti Vidyapeeth Medical College and Hospital, Sangli, Maharashtra, INDIA. Email: sunshineshilpa@gmail.com
Abstract This prospective comparative study was conducted to study and compare the perioperative haemodynamic and electrolyte changes when 1.5% Glycine and sterile distilled water is used as an irrigation fluid for transurethral resection of prostate (TURP) surgery. 100 patients of benign prostatic hyperplasia undergoing TURP of ASA Gr I,II under spinal anaesthesia were studied in two groups. Group 1(n=50) received normothermic sterile distilled water and Group 2(n=50) received normothermic Glycine 1.5% as irrigation fluid. Heart rate, mean arterial blood pressure, oxygen saturation, E.C.G findings were noted down at every 10 min. Observational record of shivering and other untoward events was kept. Post operatively serum sodium, potassium and haemoglobin and haematocrit were checked at 2and 6hrs interval. Key Words: TURP, distilled water, Glycine, haemodynamic change, electrolyte change.
INTRODUCTION Introduction- TURP is the second most common surgical procedure performed in males above 50 yrs of age for benign prostatic hyperplasia (BPH) and prostatic carcinomas. This population may suffer various comorbidities related to age such as COPD, ischaemic heart disease, diabetes, myocardialdys function,and chronic renal problems etc. TURP is an endoscopic procedure requiring large amount of irrigation fluid for visualisation, to dialate the mucosal spaces, to remove blood and, tissue debris. This irrigation fluid eventually gets absorbed into systemic circulation through opened venous sinuses. Absorption of large volume of fluid may lead to wide range of cardiovascular, nervous and other symptoms. Unnoticed and untreated clinical signs and symptoms may lead to severe cardio-pulmonary, renal, haematologic and neurologic dysfunction collectively known as TURP syndrome. Perioperative morbidity and sometimes mortality of this procedure depends on many factors such as patient's existing clinical condition, type of anaesthesia, surgical duration, prostatic gland tissue, hydrostatic pressure used and most important is type and volume irrigation fluid used. Ideal irrigation fluid should be clear, transparent, isotonic, electrically inert, nontoxic, non-metabolised and also cheap. There are many fluids available with unique pharmacological properties and systemic manifestations of each. Anaesthesiologist should know the type of irrigation fluid used to monitor and treat the adverse events. Distilled water has many qualities of a ideal irrigationfluid including low cost but due to hypotonicityit causes dilutionalhyponatremia, haemolysis, haemoglobinaemiarenal failure and CNS symptoms like confusion, convulsion and coma. Distilled water is associated with TURP syndromeif absorbed in large volume. Glycine (2.25%, 1.2%, 1.5% ) is a nonessential amino acid.1.5 % glycine is isotonic with osmolarity of 230mOsm/Lis less associated with TURP syndrome but postoperative visual symptoms like transient blindness are reported. Metabolism of Glycine may cause hyperammoniemia and hyperoxaluria. Important advantage of glycine is less haemolysis and renal failure. Sorbitol(165mOsm/L) causes hyperglycemia and lactic acidosis. Mannitol 3.5% (275mOsm/L) may cause osmotic diuresis. It is costly andnot advisable in renal disease patients. Cytal a mixture of mannitol and sorbitol is not available in India. R. Land N.S not useful due to their electricconductive ability. In India distilled water and 1.5% Glycine are most commonly used irrigation fluid for TURP surgeries. We attempted to study and compare study haemodynamic and electrolyte changes when distilled water and Glycine 1.5 % is used as irrigation fluid in 100 patients undergoing TURP surgery under spinal anaesthesia.
MATERIAL AND METHODS This prospective, randomised, comparative, double blind study was conducted on100 male patients of benign prostatic hyperplasia with ASA Gr I,II undergoing elective TURP surgical procedure for BPH under spinal anaesthesia with adequate starvation and informed consent were studied in this study. Clearance from Ethical Committee of Institution was obtained. Sample size was decided by statiscian. All patients were evaluated preoperatively and investigations including haemoglobin, complete blood count, BUN, serum creatinine, blood sugar, serum electrolytes-sodium and potassium, prostate gland size were noted. E.C.G findings recorded. Patients with existing cardiac, pulmonary, renal or spine problems were excluded from study. After confirming adequate starvation and informed consent, intravenous line was secured. Contineous monitoring of pulse rate, blood pressure, oxygen saturation, E.C.G noted preoperatively. Patient were preloaded with 10 ml/kg ringer lactate. Patient were premedicated with Inj. Glycoyrrolate 0.04mg/kg intravenously and ondansetron 0.1 mg/kg. Under all aseptic precautions central neuroaxial blockade was performed with 0.5% hyperbaric Bupivacaine 2.5cc at L4-5 interspace with 25 G spinal needle in sitting position. After confirming analgesia level up to T10 dermatome patients were positioned in lithotomy position and TURP surgery was started. Hydrostatic pressure was kept same for all patients i.e. 60 cm of H2O above the pubic symphysis of patients. Patients were randomely divided by lottery method into two groups by surgeon by lottery method. Group 1(n=50) received normothermic sterile distilled water in a steel container as an irrigation fluid. Group 2(n=50) received normothermic Glycine 1.5% in a steel container as an irrigation fluid. Investigator anaesthesiologist did not know the type of irrigation fluid. Intraoperatively heart rate, mean arterial blood pressure, oxygen saturation, E.C.G findings noted down at every 10 min. Observational record of shievering was noted and graded as +,++,+++ At the end of surgery details of duration of dissection time, blood loss, total amount of irrigation fluid were noted. All patients were shifted to S.IC.U for 24 hours. Post-operatively serum sodium, potassium and haemoglobin were checked at 2 and 6hrs interval. Any untoward cardiorespiratory and neurolgical or other symptoms were noted, evaluated and treated accordingly. At the end of study all parameterscompiled and analysed using software–SSEP 22.Quantitative and qualitative tests were applied .P value<0.001 was considered as significant RESULTS AND OBSERVATION
Table 1:
Table 2:
Table 3: Table 4:
Table 5:
Table 6:
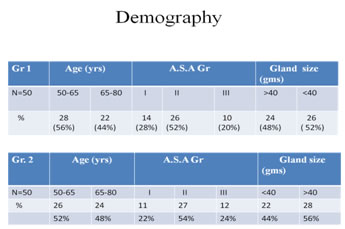
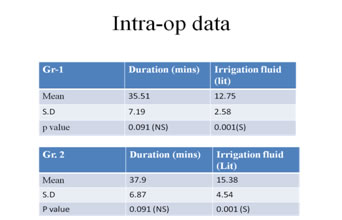
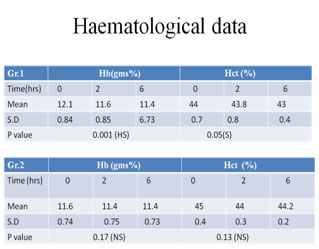
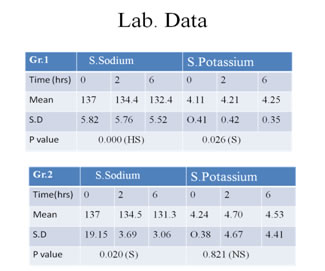
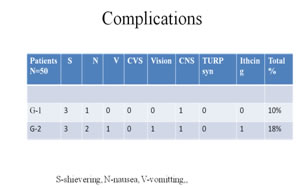
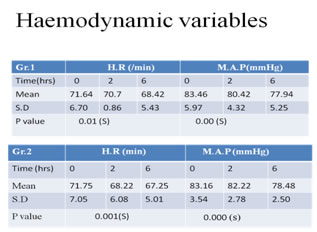
All demographic data were comparable. The age ranged from 55 -72 years (60.6±4.8) in distilled water group and 52-75 years (58.8±6.1) in 1.5% Glycine group. The weight of the patients ranged from 58-72 kg (65±2.2)in distilled water group and 60-70kg (64±2.5)in 1.5% glycine group. In distilled water group 14 (28%), 26 (52%), 10 (20%) patients belonged to A.S.A –I, II and III respectively. In 1.5% Glycine group 11(22%), 27(54%), 12(24%) patients belonged to A.S.A-I,II,III respectively. The mean amount of prostatic tissue resected was 78.15gms(±8) in distilled water group and 80.08gms (±6) in Glycine group. The mean prostatic resection time in distilled water group was 45.52(±7.19) minutes and in Glycine group it was 50.90 (±6.87)minutes. The mean amount of distilled water used as an irrigation fluid was 12.75 (±2.58) litres in group 1 and mean amount of 1.5 % Glycine used as an irrigation fluid was 15.38(4.54) litres in group 2. We compared the perioperative haemodynamic changes like heart rate, mean arterial blood pressure, E.C.G changes. Preoperative heart rate in distilled water group was 67.62(±7.8) beat/min and in Glycine group it was 70.35 (±5.8)beat/min. we observed significant decrease in heart rate after spinal anaesthesia up to 15 minutes (55.23±4.5 and 62.25±6.3 in group1 and 2 respectively)but then significant change in heart rate was not observed. Both study groups showed significant decrease in MBP (83.16±5.8 mmHg in group 1and 78.48 ±2.5mmHg in group 2after15 minutes of spinal anaesthesia. There after we did not observe fall in MBP. In group 1, we observed highly significant decrease in serum sodium after 2 hrs of surgery(134.43±5.6 mmol/l)and (132.35±5.52mmol/l) after 6 hrs. In group 2,significant fall in serum sodium level (134.58±3.69mmol/l) after 2 hrs and after 6 hrs (131.32±3.06mmol/l).Serum potassium level was significantly increased in group 1(4.21±0.41 mmol/l) after 2 hrs and (4.25±0.42mmol/l) after 6 hrs of surgery. In group 2 changes in serum potassium level was not significant (4.24±0.38mmol/l after 2 hrs and (4.70±4.67 mmol/l after 6 hrs).We also studied changes in postoperative haemoglobin in both study groups. Group 2change in haemoglobin level was not significant (11.44±0.73g/dl) whereas in group 1 significant fall in haemoglobin level (11.60±0.90) was observed. Hematocrit assessment was done and in group 1 showed nonsignificant fall after 2 hrs (44±0.3%) whereas group 2 had significant fall in postoperative haematocrit level(43.8±0.8%). None of the patient in any group required blood transfusion. In group 1,total complication rate was 10%,3 patients had shivering,1 patient complained of nausea,1 patient had one episode of vomiting. In group 2,complication rate was 18 %,three patients had shivering,2 patients complained of nausea and 2 patients had vomiting, one patient complained of blurred vision which was transient and disappeared without any specific treatment. One patient developed itching which was treated with antihistaminics
DISSCUSSION Transurethral resection of prostate (TURP) is one of the most commonly performed surgical procedure for benign prostatic hyperplasia. This procedure is minimally invasive procedure which requires continuous irrigation of fluids which can easily enter into systemic intravascular space leading to intravascular fluid, electrolyte and osmolaritychanges. Complications depend upon type and volume of fluid absorbed. Clinical manifestation may range from mild to severe, are together known as TURP syndrome. Early and milder signs are confusion, restlessness, nausea,vomiting .If unnoticed and untreated may lead to hypertension, bradycardia, siezures, hypotension, arrhythmia, coma and cardiac arrest. One or many of above said complications are seen in 2.5-20% patients undergoing TURP and perioperative mortality rate is 0.5-5%11. Both glycine and distilled water are associated haemodynamic changes when used as irrigation fluids. Moharari et al reported hypotension in 8.3% patients, hypertension in 7.8% patients when water was used as irrigant7. Olsson et al studied Glycine as irrigant and ethanol as a tracer for fluid absorption and reported hypotension, bradycardia were more prominent symptoms than hypertension13. Kumkum et al reported bradycardia with glycine when duration of resection was exceeded 60 miutes11.We did not observe significant haemodynamic changes in both group.Fall in heart rate and mean arterial blood pressure was very well attributable to spinal anaesthesia. Several mechanisms are responsible for hyponatremia in patients undergoing TURP, such as dilution of serum sodium due to excessive absorption of irrigation fluid,loss of sodium into stream of the irrigation fluid from prostatic resection site, sodium loss into pockets of irrigation solution accumulated in periprostetic and retroperitoneal spaces, glycine stimulates the release of atrial natriuretric peptide which causes natriuresis. Water intoxication and hyponatremia are attributed as primary cause for TURP1. Hyponatremia leads to weakness, muscle twitches and convulsions. Desmond et al reported that severe hyponatremia with hypo-osmolarity is reason for life threatening cerebral and cardiopulmonary events17. We observed more significant hyponatremia in glycine group than in distilled water group. Kumkum Gupta et al reported statistically significant reduction of serum sodium levels postoperatively which was proportionate to volume of glycine used.11 Hahn et al in1990 postulated that water intoxication with hyponatremia is the primary cause of TURP syndrome.1 Postoperative hyponatremia was noticed by Chen SS et al with distilled water as irrigant for TURP.8 The uptake of 1 Lit of fluid within 1hr corresponds to an acute decrease in serum sodium concentration of 5-8 mmol/l4. Symptoms of hyponatremia develops when serum sodium concentration decreases below 120 mEq /L. Absorption of more than 3 liter of fluid is hazardous. Severe hyponatremia leading to hypoosmolarity may be life threatening with cerebral or cardio-pulmonary complications. Veena et al used Ethanol 1% as marker and found good correlation between rising EB ethanol levels and hyponatremia and suggested as safe and effective noninvasive method to monitor fluid absorption during endoscopic procedure12. In our study, distilled water group did not show significant changes in serumpotassium level but significant hyperkalemia was observed in glycine group. Serum potassium level never reached above 5 mmol/lin our study. Serum potassium more than6 mmol/l is evident byclinical manifestation and E.C.G abnormalities, such as tall T waves, prolonged QRS complex and PR interval and also ventricular fibrillation. Kumkum Gupta et al found significant post operative transienthyperkalemia with 1.5 % glycine; hyperkalemia was proportionate to volume of irrigation fluid used, duration of procedure, and volume of proststate gland used. Increased serum potassium level was also reported by Hahn et al during absorption of 1.5 % glycine into systemic circulation.1 Inability of glycine to maintain isotonicity of plasma was attributed for hyperkalemia. Ayman et al however observed insignificant fall in serum potassium level in glycine group. Distilled water is clear, cheap, electrolyte free and nontoxic irrigation fluid but as it is a hypotonic solution large amount of absorption leads to haemolysis. The use of hypotonic fluids may lead to acute hypo-osmolar hyponatremia which can be fatal if not treated immediately. Madhav et al reported a case of acute intravascular hemolysis leading to renal failure when distilled water was used as a irrigant(15.)Inour study we noticed non-significant fall in haemoglobin in distilled water group, but haematocrit assessment showed non-significant changes in both groups. We did not require to transfuse blood to any patient. Chen SS et al observed haemolysis in 47.6% patients when distilled water was used as an irrigation fluid. They reported increase inplasma haemoglobin ad serum LDH.8 They concluded haemolysis was significant especially in patients with large prostate and longer resection time. Shin HC et al observed significant fall of blood Hct with distilled water. They proved as distilled water as safe irrigation fluid with monitoring of blood loss10 One of patient in glycine group complained of blurred vision which was transient. Blurred vision was resolved after 10 hrs. Studies reveal that Glycine is associated with cardiovascular and central nervous system abnormalities like fixed and dilated pupils, transient blindness, nausea and vomiting and muscular in co-ordination. Hyperammonemia and hyperglycinemia was suggested as cause for visual disturbances by Ovassipian et al in patients undergoing TURP procedure. Bansal et al reported a case of transient blindness which resolved after 24 hrs with glycine as irrigation fluid for TURP.6 Wang et al monitored ocular evoked potential and hypothesised that elevated glycine levels directly contribute to visual disturbances16. Total complication rate was 10%in distilled water group and 18% in glycine group .Moharari RS et al observed vomiting in 2.8% patients and nausea in 6.4% patients with distilled water as irrigant for TURP procedure.(7) In our study we noticed nausea in 2 patients and vomiting in 1 patients with distilled water. Moharari in their study concluded that distilled water is a safe irrigation fluid.7 None of the patient in glycine or distilled water group developed TURP syndrome in our study. Olsson et al in their study, Using ethanol as a tracer for fluid absorption, observed progressive increased incidence and severity symptoms of TURP syndrome proportionate to volume of glycine absorbed.(13) Nausea, vomiting, confusion, bradycardia, hypotension were observed. Madsen et al studied and stated that hydrostatic pressure at prostatic bed i. e height of fluid column is important factor to decide rate of fluid absorption .We had fixed the irrigation fluid column height at 60 cm. Thus we observed highly significant hyponatremia, significant hyperkalemia and highly significant reduction in haemoglobin level in postoperative period when distilled water was used as irrigation fluid whereas significant hyponatremia was noticed with glycine 1.5% glycine.These electrolyte changes were benign. Glycine 1.5% was associated with complications such as nausea-2 patients, vomiting 2 patients, blurred vision – 1,allergic reaction -1 patient. No significant haemodynamic changes were observed in both groups. CONCLUSION Glycine 1.5% and sterile distilled water both are safe irrigation fluids for transurethral resection of prostate surgery provided vigilant monitoring for haemodynamic and electrolytes and haemoglobin changes. Considering easy availability and low cost sterile distilled water is better option in developing country like India.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.