 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content Volume 8 Issue 1 - October 2018
Spinal epidural with bupivacaine 0.5% alone and bupivacaine 0.5% with fentanyl 1mcg/kg in prolonging the duration of intra-operative analgesia
M Dakshinamoorthy1, D Harishprabhakaran2*
1Professor and HOD, 2PG Student, Department of Anaesthesiology, Rajah Muthiah Medical College and Hospital, Annamalai University, Chidambaram, Tamil Nadu, INDIA. Email: harishbeastgang@gmail.com
Abstract Objectives: To compare the study and efficacy of bupivacaine versus bupivacaine with fentanyl in prolonging the duration of intraoperative analgesia. Study Design: Randomized controlled double blinded study. Materials and Methodology: A fifty American society of anaesthesiologists of category I and II undergoing for elective lower limb surgery under combined spinal epidural anaesthesia were studied in this prospective randomized double blinded study. First group I(n=25) was given inj.bupivacaine 0.5% intrathecally with epidural topup of 0.5% bupivacaine was given and Group II (n=25) was given inj. Bupivacaine 0.5% intrathecally with epidural top up of bupivacaine 0.5% with fentanyl 1mcg/kg. Vitals , duration of analgesia ,duration of blockade and complications were analyzed both intraoperatively and postoperatively. Results: The mean two segment regression time was found to be 147.00 in group l patients and 150.80 in group II. The two segment regression time in both the groups were comparable. The mean duration of intra operative analgesia was found to be 200.20 mins in group I and 293.20 in group ll patients. The 'P' value was <0.001 which was statistically significant. The group l patients had 56.60 mins more post-operative analgesia compared to group ll. In the group ll,17 patients got highest sensory block of T6 compared to 3 patients in group I. In the group ll, 5 patients got highest sensory block of T7 compared to 7 patients in group I .In the group ll,3 patients got highest sensory block of T8 compared to 12 patients in group I. AND 'P’ value is below 0.01 which is statistically significant. Group ll patients the 'P' > 0.005 statistically insignificant. Conclusion: Its is concluded that subarachnoid block with 0.5% bupivacaine and 1mcg fentanyl is a more safer and better option for patient undergoing elective lower limb surgeries. Key Word: bupivacaine.
INTRODUCTION “Egotism is the anaesthetic that dulls the pain of stupidity” Central neuraxial block has certain advantages that have made it a worthy alternative to general anesthesia in lower limb and lower abdominal surgeries. Compared to general anesthesia , central neuraxial block is associated with certain advantages like less blood loss , decreased incidence of deep vein thrombosis , conscious patients with normal airway reflexes , reduced surgical stress resulting in reduced catecholamine levels , improved ambulation and reduced cardio- respiratory complications. The two common central neuraxial blockades are epidural and subarachnoid anaesthesia. Combined spinal epidural anaesthesia, the singularity lies in its ability to combine the rapidity, density and reliability of the blockade with the flexibility of epidural block to titrate a desired sensory level,vary the intensity of the block,to control the duration analgesia and to deliver both intraoperative and postoperative analgesia The use of neuraxial opioids has dramatically increased in recent years , augmenting the analgesia produced by local anesthetics by directly binding to opiate receptors. Animal studies have also indicated that opioids and local anaesthetics administered epidurally have a synergistic analgesia effect. The synergistic action of morphine and local anaesthetics is well known. Fentanyl is phenylpiperidine derivative,synthetic opioid agonist which is 75-125 times more potent ,800 times more lipid soluble and may have advantages over morphine because of it’s rapid onset of action and superior intra -operative analgesia. Recently, preservative free fentanyl has become available making it applicable to central neuraxial block. The present study is to compare the effects between 0.5% bupivacaine alone and 0.5% bupivacaine with fentanyl 1 ug/ kg administered through lumbar epidural space in patients undergoing elective lower limb orthopedic surgeries . The intensity of blockade, hemodynamics, respiratory parameters and the intra – operative analgesia were analyzed.
MATERIALS AND METHODS Fifty American society of anesthesiologists of category I and II patients of both the sex scheduled for elective lower limb surgeries and are taken up for this study, after approval from the ethical committee of the institution. Patients with severe hypovolemia, heart disease, bleeding diathesis, increased intracranial tension, spinal deformities, sepsis and local infections were excluded from the study. Written and informed consent was obtained from each patient. Patients were randomly allocated into two groups. All the patients , taken up for study were given premedication with injection glycopyrrolate 0.2 mg , injection diazepam 5 mg by intramuscular route , 45 minutes before starting of the anesthetic procedure . 50 patients were divided randomly into 2 groups of 25 each . All the patients were cannulated with 18G intravenous cannula and preloading was done with RL 15 – 20 ml / kg body weight over 20 minutes prior to induction of block. In Group I receiving subarachnoid blockade with bupivacaine 0.5% and epidural topup with bupivacaine 0.5%.In group II,patient receives subarachnoid blockade with bupivacaine 0.5% and epidural topup with bupivacaine 0.5% +fentanyl 1mcg/kg. On arrival at operation theater, the procedure explained to the patients. Intravenous fluids was on flow . Monitors connected were non- invasive blood pressure, pulse oximeter and electrocardiogram. Resuscitation equipment was checked and kept ready. Baseline vital signs were recorded. In all patient using an aseptic technique, In sitting position 2ml of 1% lidocaine infiltered into L3-L4,L4-L5 intervertebral space using 25G hypodermic needle. The epidural space was identified by the loss of resistance technique using a 18G touhy needle, epidural catheter was inserted and secured in position in aseptic manner. The patient was positioned supine immediately. Precalculated dose of the drug was injected slowly. Group l patients received 2.5 cc of 0.5% Bupivacaine and Group ll patients received 2.5cc of 0.5 % Bupivacaine intrathecally. Group I patients received epidural top up with Bupivacaine 0.5% alone after 1 hour and Group ll patients received epidural top up of Bupivacaine 0.5% and fentanyl 1 mcg/ kg. At the end of the surgical procedure , patients were shifted to recovery room and monitored for 2 hours postoperatively after the patients were shifted to postoperative Ward. All the patients were monitored for heart rate , respiratory rate , oxygen saturation and blood pressure in the preoperative , intraoperative and post operative period for a period of 3 to 5 hours. Intraoperatively and postoperatively the following parameters were studied.Dermatomal sensory blockade to pinprick was evaluated, maximum level of impaired sensation noted and duration of analgesia and Intensity of motor blockade using modified bromage scale, degree of pain intra operatively was evaluated by Visual Analogue Scale. Rescue analgesia time was recorded in all the cases in both the groups. Using Ramsay sedation scale, sedation was assessed in all the cases. All neurological deficits, bowel and bladder dysfunction were noted for 72 hours in the postoperative period. All the parameters were subjected to appropriate statistical analysis before inference was drawn.
OBSERVATION AND RESULTS Table 1: Comparison of onset of sensory block, two segment regression and duration of block between two groups
Among two groups , group - ll patients show quicker onset of action with mean onset time being 6.40 min and long intra-operative analgesia which extends well into post-operative period. Showing significant action of fentanyl additive to local anaesthesia. There was no significant deviation in two segment regression time between the two groups.
Table 2: Percentage of level of sensory block in both the groups
Among the patients compared 17 patients of group-2 had highest level of sensory blockade to T6 compared to 3 patients in group-1 showing Bupivacaine with fentanyl having highest level of sensory blockade
Table 3: Percentage of motor block in both the groups
In group-l, 9 patients had incomplete motor blockade while 16 patients had complete blockade as compared to 6 patients with incomplete blockade and 19 patients had complete blockade in group-ll. Motor blockade level was similar in both groups. Table 4: Comparison of pulse rate at various intervals between two groups (Beats / min)
The mean of pulse rate significantly differs at different time periods in both groups of patients.
Table 5: Comparison of mean arterial pressure between two groups at various intervals (mm of Hg)
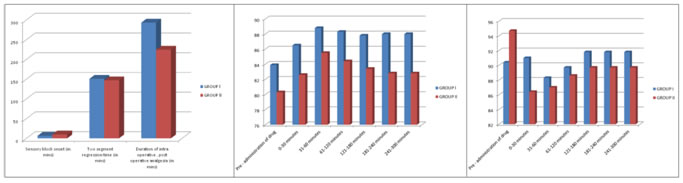
Since the interaction effect between period and group was found to be significant , it infers that the changes in mean blood pressure was significantly different in group ll patients than in group I patients i.e , in group ll patients the normal range of mean arterial pressure was well maintained. The Mean arterial pressure shows the normal range is well maintained in group ll patients than in group I showing good control with fentanyl and Bupivacaine than Bupivacaine alone. Figure 1 Figure 2 Figure 3 Figure 1: The bar diagram showing the onset of sensory block, two segment regression time; Figure 2: The bar diagram showing the pulse rate at various intervals between two groups (beats / min); Figure 3: The bar diagram showing the mean arterial blood pressure between two groups at various intervals (mm of hg) DISCUSSION Pain is one of the commonest symptom that lead a patient to seek medical advice and whatever be the cause , it demands relief , it’s importance was evidenced by Sydenham in 1980 “ among the remedies which had pleased almighty GOD to give man to relieve his suffering , none is so universal and so efficacious as opium “.From early 1980’s the practice of epidural analgesia for postoperative pain relief had set in . Earlier it was routinely used for orthopedic surgeries . Later it was used routinely for surgical and obstetric procedures. At present , it is practiced for thoracotomies as well. Badner et al ( 1994) suggested that addition of 0.125% Bupivacaine improves the analgesia of epidural injection of fentanyl 10 mcg/ml when used in abdominal or thoracic surgeries. Dhalae, shelgaonicar et al (2000) compared epidural Bupivacaine with fentanyl of three different doses 25/50/75 mcg and epidural 0.5% Bupivacaine alone for orthopedic surgeries. The observed that 50mcg fentanyl with 0.5%Bupivacaine is a better choice. Casimiro et al (2008) allocated 96 patients to receive levobupivacaine 5mg with fentanyl 100mcg (n=49) and bupivacaine 5mg with fentanyl 100mcg (N=47) . They observed a trend in levo bupivacaine group , which had a lesser motor blockade. In our study we compared the effects of 0.5% bupivacaine alone and 0.5% bupivacaine with fentanyl 1mcg/kg through lumbar epidural for cases of elective lower limb surgeries after one hour. The mean onset of sensory block was 2.0 mins . Our result is compared with Johnson at al (1989).The mean two segment regression time was found to be 147.00 in group l patients and 150.80 in group ll patients. The 'P' > 0.005 statistically insignificant. The two segment regression time in both the groups were comparable as reported by Singh H and Yang J et al. The mean duration of intra operative analgesia was found to be 200.20 mins in group I and 293.20 in group ll patients. The 'P' value was <0.001 which was statistically significant. The group l patients had 56.60 mins more postoperative analgesia compared to group ll. Similar results were observed by Rutter Dv et al (1981),Johnson et al (1989) , dhale et al (2000).In the group ll,17 patients got highest sensory block of T6 compared to 3 patients in group I. In the group ll, 5 patients got highest sensory block of T7 compared to 7 patients in group I .In the group ll,3 patients got highest sensory block of T8 compared to 12 patients in group I. AND 'P’ value is below 0.001 which is statistically significant. The group ll patients had highest level of sensory block compared to group I. Our results were comparable to the Johnson et al (1989).In group I , 9 patients had incomplete motor blockade while 16 patients had complete blockade as compared to 6 patients who had incomplete blockade while 19 had complete blockade in group ll. The pulse rate, mean arterial pressure were maintained within normal range in both groups . These results were comparable with the studies conducted by T.A. Torde et al. 5 patients in group I and 5 patients in group ll had hypotension. Other complications such as bradycardia , respiratory depression, postoperative nausea and vomiting, pruritus and urinary retention were not found in both groups as reported by MA chamay et al.The principal findings of this study are that the addition of 1 mcg/kg fentanyl to hyperbaric 0.5% bupivacaine intensifies the sensory blockade and increases the duration of sensory blockade. Opioids and local anesthetics exert their antinociceptive effect in the spinal and by different mechanism. The mu agonist fentanyl exerts it’s action by opening the k+ channels and reducing the ca2+ influx , resulting in inhibition of transmitter release. The mu agonist also have a direct post synaptic effect, causing hyper polarization and a reduction in neuronal activity. Local anaesthetic, bupivacaine acts mainly by blockade of voltage gated Na+ channels in the axonal membrane and possibly a further effect on presynaptic inhibition of ca2+ channels. A combination of these effects may explain the observed synergism between bupivacaine alone and bupivacaine with fentanyl in our study. The synergism is characterized by enhanced somatic analgesia without effect on degree on the level of local anaesthetic induced sympathetic or motor blockade. Many studies demonstrated this synergism and prolongation of sensory blockade with fentanyl addition to either lidocaine or bupivacaine or levo bupivacaine as reported by vinitha Singh, casimiro et al.
CONCLUSION From this study , we conclude that 0.5% bupivacaine with fentanyl 1mcg/kg through lumbar epidural for elective lower limb orthopedic surgeries has got the following advantages than epidural 0.5% bupivacaine alone.
Fentanyl in combination with bupivacaine administrated epidurally has advantages over bupivacaine alone in increasing the duration of intraoperative analgesia without producing any respiratory depression or hemodynamic changes. In clinical practice fentanyl can be used epidurally as a safe adjuvant along with bupivacaine
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.