 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 10 Issue 3 - June 2019
Effect of walking on Fasting Blood Sugar and HbA1c in type 2 Diabetes Mellitus
R Sirisha1*, Pitta Paramjyothi2
1Associate Professor, Department of Physiology, Guntur Medical College, Guntur, Andhra Pradesh, INDIA. 2Professor and HOD, Department of Physiology, Government Medical College, Siddipet, Telangana, INDIA. Email: sirisha.mahesh33@gmail.com
Abstract Background: There is increased evidence of overweight, obesity and pre-diabetes continued to rise with decreased physical activity in the community. Aims and Objective: The aim of the study is to introduce regular physical activity in Type 2 diabetic patients and its potential effects in controlling Fasting Blood Sugar and HbA1c status. Type 2 Diabetic patients with regular treatment over five years without complications were selected to measure their Fasting Blood sugar and HbA1c levels before and after 30 minutes of regular walking for 12 weeks. There is a change in Fasting Blood Sugar and HbA1c levels with p-value <0.001 and <0.05 respectively. Regular physical activity like walking prevents and delays long term complications of diabetes, decreases stress and creates a sense of well-being. Key Word: Fasting Blood Sugar HbA1c Type 2 Diabetic patients Walking.
INTRODUCTION Walking as a regular physical activity in diabetic patients is the most crucial goal of the trail. Most of the studies indicated that many Type 2 Diabetic patients do not follow the prescribed exercise regimen. Long-term continuation of exercise in people with diabetes become a remote possibility. Motivation and reinforcement made the patients to follow the exercise regimen. After counseling the most frequent activity chosen by the patients is walking. It can be implemented quickly every day. Reasons for implementation being are to get a refreshing feel and not only because of the advice by a physician. Exercise requires major metabolic, cardiovascular adjustments to increase the supply of fuels, oxygen to working muscles to maintain the brain and other vital organs. Walking has multiple positive benefits1. It results in lowering plasma glucose during, following exercise and there will be increased sensitivity and response to insulin in skeletal muscle. While walking for extended periods muscles are active only for a fraction of each step and cause relatively little fatigue. Walking 2.5 km for 30 minutes fits well with the current exercise recommendations.
MATERIALS AND METHODS: The work was carried out at Government General Hospital Guntur, General Medicine Out-Patient department and Government Medical College Guntur in the department of Physiology. Prior to the study each patient was informed about the protocol and their written consent was obtained. We selected total number of 25 male patients with Type 2 diabetes over five years and exercise therapy in the form of brisk walking was advised to them. All the patients were followed the exercise for 12 weeks duration. An adult walking at a comfortable pace moves with a velocity of about 80 meters/minute generates a power output of 150-170 watt/step. Rough indicator very useful in assessing the intensity of exercise is "The Walk and Talk Test." During the safe and comfortable walk the person should be able to continue a conversation while walking. The Fasting Blood Sugar (FBS) and HbA1c levels were taken before and after 30 minutes of walking and after 12 weeks continued therapy.
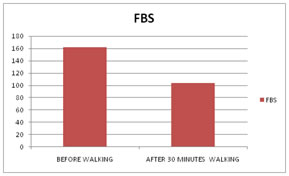
RESULTS A total of 25 Type 2 Diabetic patients with regular treatment over five years without complications were selected to measure their FBS and HbA1c levels before and after 30 minutes of regular walking for 12 weeks. FBS declined and HbA1C levels improved after walking. Comparison between Mean and Standard Deviation of FBS and HbA1c before and after 30 minutes walking for 12 weeks showed improvement in the control of Diabetes was directly proportional to the degree of hyperglycemia before training. The data obtained was analyzed using unpaired students t-test. Table 1: Comparison of fbs before and after 30 minutes walking
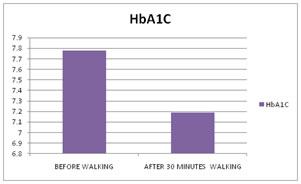
Table 2: Comparison of HbA1c before and after 30 minutes walking
DISCUSSION The Entry of glucose into the cell occurs by the process of facilitated transport mediated by a specific glucose transport protein in the plasma membrane. Regular exercise as walking enhances insulin binding to its receptor on the muscle cell membrane. Insulin is a modulator of glucose transport during exercise and magnifies its effect2,3. Insulin causes translocation of glucose transporters from the intracellular membrane to the plasma membrane in muscle. The increased membrane glucose transport capacity is caused by the recruitment of glucose transporters (GLUT-4) to the sarcolemma and t-tubules. During muscle contractions glucose transport seems to be regulated by feed forward Ca2+ dependent signal that triggers GLUT-4 translocation in contracting muscle and protein kinase C, Nitric Oxide, glycogen and activated protein kinase as a metabolic feedback signal4.The use of Free Fatty Acids by muscle also increases during exercise. Generally the importance of Free Fatty Acids as a fuel relative to glucose increases with the duration of exercise and decreases with increased intensity of exercise. Regular mild physical exercise as walking plays a role in controlling Type 2 Diabetes. It is observed that physical activity increases sensitivity to insulin and regular endurance exercise induces weight loss and improves glucose tolerance. Exercise and insulin interact synergistically in stimulating total glucose utilization and carbohydrate oxidation. The magnitude of insulin's suppressive effect on FFA levels and fat oxidation is increased by exercise. In a patient with Type 2 diabetes with walking as exercise there is a significant decrease in hyperglycemia during a 30 minutes period was observed.
CONCLUSION The study concludes that regular endurance exercise in the form of walking improves glucose homeostasis and may serve as an adjunct to other modes of treatment in Non-Insulin Dependent Diabetic individuals. The higher levels of physical activity are clearly associated with a lower incidence of Type 2 Diabetes. In diabetic patients at rest glucose production will be elevated and metabolic clearance is suppressed. During exercise glucose production fails to increase significantly accounting for the decline in plasma glucose. Like drugs, physical activity can be part of doctors' prescription. It is usually aimed at improving physical fitness, reducing disease risk or by treating an illness. Careful management of Type 2 Diabetes by a physician should focus not only on drugs and diet but also on regular physical exercise which reduces the requirement of medications and prolongs the longevity of life.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.