 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 11 Issue2 - August 2019 Correlation of BMI with sympathetic functions: A harbinger for autonomic neuropathy in young adults
Aparna M1, Ganashree C P2*, Devaraj M G3, Shreevijay Bevinagidad4
(1Assistant Professor, 2Professor, 3Professor and HOD, Department of Physiology} {4Associate Professor, Department of Radio-diagnosis) Basaveshwara Medical College and Hospital, Chitradurga -577502, Karnataka, INDIA. Email: draparna.bly@gmail.com
Abstract Background: Body Mass Index (BMI) is the marker for body fat content. It has been used to identify and classify individuals who are most likely to be overweight or obese. Increase in BMI (>25kg/m2) is not only risk factor for cardiac disorders but also altered autonomic functions. Aim and Objective: To assess sympathetic functions and its relationship with BMI in young adults Methods: After obtaining institutional ethical clearance , 100 healthy subjects aged between 18-40 years were selected and categorized in two groups. First group with BMI <25kg/m2 and second group with BMI >25kg/m2 consisting of fifty subjects in each group. Blood pressure (BP) response to standing (BPRS) and BP response to sustained handgrip exercise (HGE) were recorded using mercury sphygmomanometer. Results: In comparison with Group I, Group II subjects showed statistically significant increase in the Weight, BMI and Body Surface Area (BSA), Whereas resting heart rate in Group II subjects was statistically not significant. Sympathetic functions where significantly reduced in Group II subjects as compared to group I. We observed there was a negative correlation between BMI and SNS functions in group II. Interpretation and Conclusion: Increase in BMI is associated with altered sympathetic nervous system functions which can cause far-reaching adverse effects in near future, including metabolic syndrome and cardiovascular malfunction. So having a constant check on BMI helps in preventing SNS abnormalities. Key Words: BMI, Handgrip exercise, SNS,
INTRODUCTION With continued rise of standards of living, obesity is emerging as a global epidemic in both children and adults. This has been called “New world syndrome” and is a reflection of massive social, economic and cultural problems currently facing developing and developed countries.1 Obesity is the current serious public health problem with established cardiovascular comorbidities and a major cause of sudden death in developed as well as developing countries.2 BMI is a simple index of weight for height commonly used to classify underweight, normal, overweight and obesity in adults. It is defined as the weight in kgs divided by height in metres square ( kg/m2).3 WHO has set standards for overweight and obesity by defining it as BMI ≥25 kg/m2 and ≥30 kg/m2 respectively. But, the BMI cut off point for overweight (≥23 kg/m2) and obese (≥25 kg/m2 ) for Asians are lower than the WHO criteria.4 Autonomic nervous system (ANS) is a vital centre for the coordination of different body systems.5 Since ANS is involved in energy metabolism and regulation of cardiovascular system,5,6 Previous studies strongly suggest that obesity might be linked with not only higher risk factor for Cardiovascular Heart Disease (CHD) but also reduced ANS activity.7 Thus, the present study has been attempted to assess relationship between sympathetic nervous system activity and body mass index using autonomic function tests as diagnostic tools, which would thus help in detecting subclinical alteration of autonomic functions.
AIM and OBJECTIVE To assess sympathetic functions and its relationship with BMI in young adults
MATERIALS AND METHODS The cross-sectional study was carried out in 100 healthy subjects in the age group of 18 - 40 years, randomly selected among the employees of our institute. 100 subjects were divided into two groups of 50 each, with BMI<25 kg/m2(Group I) and BMI ≥25 kg/m2(Group II). The ethical clearance for the study was obtained from institutional ethical committee. Each subject taking part was explained about the purpose and procedure to be adapted in the research. All the subjects after thoroughly understanding the procedures to be adopted signed an informed consent form provided to them. The data was collected in the Research Laboratory of Department of Physiology, Chitradurga. Inclusion criteria The subjects without signs of cardiovascular, endocrinological, neurological, hematological and inflammatory diseases were selected for the study. Exclusion criteria
Guillean Barre syndrome, Poliomyelitis, Diphtheria, Tuberculosis, Syphilis, Amyloidosis, Chronic renal failure. Sample size The study was conducted on 100 healthy employees of our institute. Sample size calculated by the following formula: n=DEFF.Np(1-P)/d2.(N-1)+P(1-P) using OPEN EPI and SPSS Software. Z2 1-α/2. Method of collection of data The subjects were asked to relax in supine position for 30 minutes in the laboratory. The tests were performed only after complete relaxed physical and mental state of the subjects. All the subjects were subjected to recording of their physical anthropometry, various physiological parameters and autonomic function parameters. Height was recorded using vertical height scale, and weight measured using weighing machine (Dolphin Company), ECG machine (RMS Company) was used to record ECG changes, Blood pressure (BP) was measured with the help mercury sphygmomanometer (Diamond) and Hand grip dynamometer (INCO Ltd) used to study effect of handgrip exercise on BP. Recording of Autonomic Function Parameters The following cardiovascular autonomic function tests were performed. Results of the tests were expressed as ratios and differences which have been accepted by Ewing and Clarke.8
A. The sympathetic activity was assessed by: 1. Blood pressure response to standing: The subject rested comfortably in supine position for 15 minutes. And then thev subject was asked to stand up unaided and remain standing. Systolic blood pressure (SBP) was recorded in resting supine position and again immediately when he stands up. And the difference in SBP was noted. Fall in SBP of 10 mm Hg or less is taken as normal response.8
2. Blood pressure response to sustained Hand grip exercise: The subject was asked to sit comfortably in chair. Initially the subject was asked to exert maximal hand grip strength on hand grip dynamometer with dominant hand. First the maximum voluntary contraction (MVC) is determined and then the subject was asked to exert 30% of MVC for 5 minutes (at least for 3 min) with dominant hand. Diastolic blood pressure was measured in the non-dominant hand at rest and at one minute interval during hand grip. The maximum rise in diastolic BP during 30% of MVC over the resting diastolic blood pressure was noted. Grading (Ewing and Clarke)8 and autonomic function score of the results: Normal Borderline Abnormal Score 0 1 2 1. H.R response to Valsalva maneuver >1.21 1.11-1.20 <1.10 2. H.R response to deep breathing >15bts/min 11-14bts/min <10bts/min 3. H.R response to standing >1.04 1.01-1.03 <1.0 4. BP response to standing <10mmHg 11-29mmHg >30mmHg 5. BP response to sustained hand grip >16mmHg 11-15mmHg <10mmHg
Criteria for grading autonomic function as whole9 Scores < 3 Normal autonomic function > 3 and < 8 Borderline dysfunction > 8 to 10 abnormal function Statistical Analysis All statistical analysis was done by using SPSS software version 17. Values expressed in terms of Mean ± Standard Deviation (Mean ± SD). Chi- square test was applied to estimate the difference between Group I and Group II. Independent ‘t’-test was used to compare the variables between the 2 groups. Correlation between various autonomic function parameters and BMI is done by Pearson’s correlation coefficient.
RESULTS All the results were expressed as Mean ± SD. Table 1: Mean+SD Values of Sympathetic function test parameters ( BPRS and BPHG ) between Group I and Group II
⃰ p Value < 0.05 – Significant (S) and p Value >0.05 – Not Significant (NS)
Table 2: Correlation between BMI and BP response to Handgrip (BPHG)
* Correlation(negative) is significant at the 0.01 level (2-tailed)
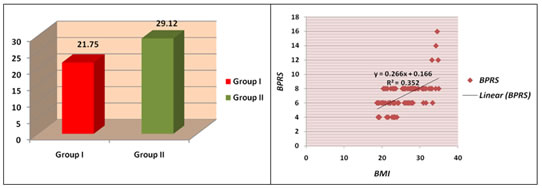
Figure 1: Showing mean BMI of two Groups Figure 2: Correlation between BMI and BPRS There is positive correlation between BMI and Blood pressure response to Standing (BPRS)
DISCUSSION A large volume of data is available as regards the indirect role of ANS in obesity (increase in BMI) but a comprehensive study of the autonomic status and its relation with BMI is not available. Our study endeavors to show the status of sympathetic nervous system and its relationship with increase in BMI in healthy adults with the help of reliable, non-invasive, and easily reproducible cardiovascular autonomic function tests by Ewing. 1. Blood pressure response to standing (BPRS): With change of posture from supine to standing the autonomic nervous system acts to produce a rise in heart rate and vasoconstriction in order to maintain blood pressure.11 In our study we found borderline fall in Systolic blood pressure on standing in group II subjects (table 1) when compared to group I subjects ( p=0.000) . Akhter et al12 also reported lower BP response to standing indicating lower sympathetic nerve activity in obese person compared to non-obese adults. Present Correlation study revealed significant positive correlation and r value is 0.269 (fig 2) between increasing BMI and Blood pressure response to standing (ie. More fall in SBP on standing ) indicating sympathetic dysfunction in the form of decrease in sympathetic activity.12 2. Blood pressure response to hand grip exercise (BPHG) : D.J Ewing et al first showed that during sustained hand grip, there was a sharp rise in diastolic blood pressure (DBP) due to increase in peripheral vascular resistance.13In our study we found decrease rise in DBP to hand grip exercise in group II subjects (table 1) and was statistically significant (p=0.000) . This decrease in blood pressure response to isometric handgrip exercise shows decrease activity of the sympathetic nervous system14 or to a lower increase in peripheral resistance to maneuvers activating sympathetic system.15 Our study shows negative correlation (r = -0.596) between increasing BMI and BPHG (table 2) indicating lower sympathetic nerve function.12 Sympathetic function test findings of our study revealed hypofunctional sympathetic ANS dysfunction in group II subjects with increase in BMI. Similar results were also observed in other studies.12,16 Kalpana et al16 also observed reduced DBP response in obese group to handgrip exercise suggestive of a reduced sympathetic activity in obese individuals when subjected to stress ; and this entail an increased susceptibility to develop cardiovascular disorders.
CONCLUSION In our study we assessed the autonomic functions in two BMI groups (Group I – BMI < 25 kg/ m2 and Group II- BMI ≥ 25 kg/ m2) and the following conclusions can be drawn:
REFERENCES
|
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.