 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 2 - November 2019
A comparative cross-sectional study of blood pressure changes in postmenopausal and premenopausal women
Padmakar Sasane1, Pandurang Narhare2*
1Assistant Professor, Department of Physiology, Lt.B.R.K.M Government Medical College, Dimrapal, Jagdalpur, Chhattisgarh. 2Professor, Department of Physiology, ESIC Medical College and ESI-PGIMSR, Joka, Kolkata, West Bengal. Email:drpandurang28@gmail.com
Abstract Background: Menopause means cessation of menses after reproductive life. Hypertension is a continuous, non-occasional state of elevated blood pressure (BP) which increases with age. Women of different ethnicity show higher prevalence of coronary artery disease and hypertension after menopause. As a consequence of longer life expectancy and modern lifestyle, the prevalence of hypertension is expected to increase. While diastolic BP starts to increase earlier. Systolic BP starts to increase after 50 years of age. Materials and Methods: This study was a cross sectional study done in Department of Physiology, Lt.B.R.K.M Government Medical College, Dimrapal, Jagdalpur (Bastar), Chhattisgarh from July 2018 to June 2019. Study was undertaken from data collected from postmenopausal and premenopausal women of similar height and weight of general population of Tokapal Block. After a detailed medical history on the basis of the following inclusion and exclusion criteria 50 postmenopausal women and 50 premenopausal women were taken. We used convenience type of sampling. It is a non-probability sampling design. Postmenopausal state was considered in women who had at least 12 months amenorrhea. Results: The systolic blood pressure in postmenopausal group was 120.54 ± 2.56 mm Hg and in premenopausal 118.45 ± 3.23 mm Hg. The diastolic blood pressure in postmenopausal group was 81.65 ± 2.23 mm Hg and in premenopausal 80.34 ± 4.02 mm Hg. Higher statistical difference in the blood pressure is observed in both systolic and diastolic blood pressures between the two different groups. There was a higher in Pulse rate (bpm) 83.16 ±1.45, Systolic Blood Pressure 120.54 ± 2.56 (mmHg), Diastolic Blood Pressure 81.65 ± 2.23 (mmHg), in postmenopausal women. Conclusion: Both systolic blood pressure and diastolic blood pressure were significantly higher in postmenopausal women than premenopausal women. Oestrogen deficiency leads to oxidative stress due to release of free radical or reactive oxygen species (ROS) which causes various pathologies like hypertension. In postmenopausal women, oxidative stress causes potential oxidative injury to cells causing diseases in this stage of life. Key Words: Hypertension, post-menopause, pre-menopause, systolic blood pressure, Pulse rate.
INTRODUCTION Menopause means cessation of menses after reproductive life.Hypertension is a continuous, non-occasional state of elevated blood pressure (BP) which increases with age. Women of different ethnicity show higher prevalence of coronary artery disease and hypertension after menopause As a consequence of longer life expectancy and modern lifestyle, the prevalence of hypertension is expected to increase.1 While diastolic BP starts to increase earlier. Systolic BP starts to increase after 50 years of age. The increase in systolic BP is of higher health risk. A higher incidence of cardiovascular and cerebrovascular diseases is observed respectively 10 and 20 years after BP increase.2A 2012 World Health Organization report shows that the rise of BP causes 51% of deaths from stroke, and 45% of deaths from coronary artery diseases.2There are sex differences in the development of hypertension.3 The National Health and Nutrition Examination Survey (NHANES) shows that, prior to 45 years of age, prevalence of hypertension is higher in men than in women. From 45 to 54 years and from 55 to 64 years of age, the percentage of hypertensive men is similar to that of hypertensive women. After 65 years of age, BP levels increase faster in women than in men.4It has been suggested that sex steroids protect fertile women from hypertension and that gonadal steroid withdrawal may play a role in the modifications of BP control.5 In fact, the role played by steroid withdrawal at menopause is still controversial.
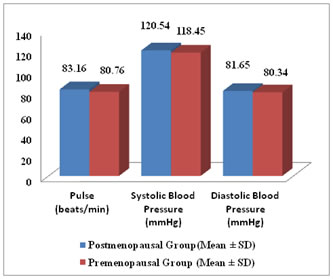
MATERIALS AND METHODS This study was a cross sectional study undertaken in Department of Physiology, Lt.B.R.K.M Government Medical College, Dimrapal, Jagdalpur (Bastar), Chhattisgarh from July 2018 to June 2019.Source of Data: Study data was collected from postmenopausal and premenopausal women of similar height and weight of general population of Tokapal Block, Bastar District, Chhattisgarh. After a detailed medical history on the basis of the following inclusion and exclusion criteria 50 post-menopausal women and 50 pre-menopausal women were taken. We used convenience type of sampling. It is a non-probability sampling design. Postmenopausal state was considered in women who had at least 12 months amenorrhea. Inclusion Criteria: Fifty post-menopausal women aged 50-55 years with active physical life and attained menopause naturally. Weight 60 to 65 kgs, Height 155-157.5 cms were measured. Normal healthy aged 35 to 40 years with height and weight matched fifty pre-menopausal women with regular menstrual cycles were taken. Exclusion Criteria: Participants with these diseases were excluded. Diseases like dyslipidaemia blood disorders, surgical menopause, hypertension, Diabetes Mellitus, thyroid disorders, renal diseases they should not have received oestrogen therapy or supportive treatment for menopausal symptoms. The height was measured using stadiometer. Clinical weighing machine was used to record weight of subjects dressed in light clothing.The BP of the subjects were measured three times in sitting position first by palpatory method and then by auscultatory method using Mercury Sphygmomanometer. Korotkoff sounds, appearance of sound (Phase I) is taken as Systolic BP, and disappearance of (phase V) Korotkoff sound is taken as Diastolic BP. Methods of Collection of Data: Women population of Tokapal Block was randomly selected with similar height and weight matched both pre and post-menopausal women were taken for study. Proforma was given to all of them. Written informed consents are taken during the face to face questionnaire interview. An examination of respiratory, cardiovascular, central nervous system and gynaecological examination was done. Statistical analysis was done by using students ‘t’ test. RESULTS The data of the healthy postmenopausal and premenopausal women is shown in table 1. Resting Pulse Rate: The [mean ± SD] pulse rate at rest in postmenopausal group groups was 83.16 ±1.45 beats/ min and in premenopausal group 80.76 ± 2.32 beats/min. Higher statistical difference is seen in the resting pulse rate between the two different groups Blood Pressure: The [mean ± SD] systolic blood pressure in postmenopausal group was 120.54 ± 2.56 mm Hg and in premenopausal 118.45 ± 3.23 mm Hg. The [mean ± SD] diastolic blood pressure in postmenopausal group was 81.65 ± 2.23 mm Hg and in premenopausal 80.34 ± 4.02 mm Hg. Higher statistical difference in the blood pressure is observed in both systolic and diastolic phases between the two different groups. There was a higher in Pulse rate (bpm) (83.16 ±1.45), Systolic Blood Pressure (mmHg) (120.54 ± 2.56), Diastolic Blood Pressure (mmHg) (81.65 ± 2.23), in postmenopausal women.
Table 1: Blood Pressure Changes in Post-menopausal Group and Pre-menopausal Group
Figure 1: Pulse rate, Systolic BP and Diastolic BP changes in Postmenopausal Group and Premenopausal Group DISCUSSION During menopausal transition blood pressure raises due to additive effect of other hormone related factors. Decrease in oestrogen levels around menopause causes an up regulation of the Renin Angiotensin System (RAS) with higher plasma renin activity. Sympathetic activity is higher in postmenopausal women than in age-matched men, especially in women who are overweight.6 Sympathetic over activity is associated with abdominal visceral fat which is strongly related to higher inflammatory markers and oxidative stress.7Zanchetti A et al (2005)8 says premenopausal women have low blood pressure than in the postmenopausal women. Also postmenopausal women develop arterial hypertension often together with changes in lipid and glucose metabolism.9 Many studies convey that production of catecholamines is raised and a clear shift of the autonomic control towards a higher sympathetic activity of the cardiovascular system. This higher sympathetic drive is closely related to the state of oestrogen deficiency as it occurs in a few days after surgical oophorectomy and is reversed by oestrogens. Metabolic changes with raised sympathetic drive occurring after the menopause, contribute to cause the metabolic syndrome. The physiological and structural changes, due to higher sympathetic drive leads to hypertension development.10, 11
CONCLUSION Both systolic blood pressure and diastolic blood pressure were markedly higher in postmenopausal women than premenopausal women. These differences may be due to lower oestrogen levels around menopause that causes an up regulation of Renin Angiotensin System (RAS) with a raise in plasma renin activity. Oestrogen deficiency leads to oxidative stress due to release of free radical or reactive oxygen species (ROS) which causes various pathologies like hypertension. In postmenopausal women, oxidative stress causes potential oxidative injury to cells causing diseases in this stage of life. Natural menopause does not immediately aggravate heart disease which may be due to both age and oestrogen deficiency.Sympathetic over activity is associated with abdominal visceral fat which is strongly related to higher inflammatory markers and oxidative stress.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.