 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 12 Issue 2 - November 2019
Comparison of anthropometric parameters among individuals with pre-diabetes and obstructive sleeps apnea
Ramya K1*, Gowri Sethu2, Dhanasekar T3
1Department of Physiology, ACS Medical College and Hospital, Chennai, Tamil Nadu, INDIA. 2Professor of Physiology, Saveetha Dental College, Chennai, Tamil Nadu, INDIA. 3Pulmonologist and sleep specialist, Summa Institute of Sleep Medicine, Chennai, Tamil Nadu, INDIA. Email: ramyakumar_2006@yahoo.co.in
Abstract Background: Assessment of anthropometric parameters is especially important when correlating a disease with obesity. It provides valuable information to diagnose a disease in advance. As India is going to become diabetes capital of the world, it is essential to diagnose the diabetes in early stages to provide adequate treatment and also to limit the prevalence of diabetes. Obstructive sleep apnea (OSA) is associated with glucose intolerance and insulin resistance. Objective: In this regard, it is essential to understand the relation between the sleep apnea and the diabetes. The present study was undertaken to compare the anthropometric parameters in individuals with pre-diabetes and obstructive sleeps apnea. Methods: The study was conducted was conducted among three groups, each comprising of 50. The participants were in the age group 30-60 years of both sexes. The participants received a detailed explanation about the procedure and their cooperation and willingness was obtained with an informed consent. The demographic status and a detailed clinical history of all the subjects were collected. Results: In the anthropometric parameters, weight, BMI & neck circumference were significantly higher in prediabetic and OSA when compared to control group. Between pre-diabetic and OSA, the three values were significantly higher in the OSA group. Height was not a significant variable among all the three groups. Conclusion: The study results support the importance and value of the anthropometric parameters in the pre-diabetes and obstructive sleep apnea conditions. Further detailed studies with higher sample size and multi center studies are recommended in this area for better understanding the relationship between these parameters, which helps to design effective treatment modalities. Key Word: Pre-diabetes, Sleep, Apnea, Anthropometric data
INTRODUCTION Assessment of anthropometric parameters is especially important when correlating a disease with obesity.1It provides valuable information to diagnose a disease in advance. As India is going to become diabetes capital of the world, it is essential to diagnose the diabetes in early stages to provide adequate treatment and also to limit the prevalence of diabetes. Prediabetes is a health condition that means your blood sugar level is higher than normal, but not yet high enough for you to be diagnosed with diabetes. Obesity, type 2 DM, metabolic syndrome, and obstructive sleep apnoea (OSA) are interrelated conditions. People having these disorders are prone to develop dyslipidemia and consequently, cardiovascular disease. An early indicator of type 2 DM is increase in insulin resistance.2,3 Insulin resistance leads to the development of hypertension, cardiovascular disease and type 2 DM. Obesity and insulin resistance are common features of both metabolic syndrome and obstructive sleep apnoea (OSA).4 Obesity has become a growing problem in developing countries and is a major risk factor for developing obstructive sleep apnoea. It was reported that the sleep apnea is related with the diabetes. OSA is associated with deregulation of glucose homeostasis.5Obstructive sleep apnea (OSA) is associated with glucose intolerance and insulin resistance. In this regard, it is essential to understand the relation between the sleep apnea and the diabetes.16The present study was undertaken to compare the anthropometric parameters in individuals with pre-diabetes and obstructive sleeps apnea.
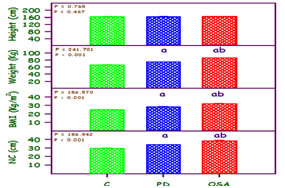
MATERIALS AND METHODS Study design: The present study was a cross-sectional study. Study setting: Department of Physiology, ACS Medical College and Hospitals, Dr. MGR Educational and Research Institute University, Summa Institute of Sleep Medicine and Saveetha Institute of Medical and Technical Sciences, in Chennai, Tamil Nadu, India, during January 2015–December 2016. Study participants: The study was conducted was conducted among three groups, each comprising of 50. The participants were in the age group 30-60 years of both sexes. The participants received a detailed explanation about the procedure and their cooperation and willingness was obtained with an informed consent. The demographic status and a detailed clinical history of all the subjects were collected. Sample size : The sample size was estimated assuming 20% difference among the mean 25% standard deviation, 3group (e, PD, OSA) 90% power, 5% significance level. The estimated sample size 41 and it was rounded to 50 each for the three groups. Sample size was estimated by SigmaStat 13.0 (Systat software, USA). Sampling technique: The method of sampling technique used quasi-random sampling. Anthropometric assessment: The subjects underwent comfort evaluation of the anthropometric measures such as body weight, height, body mass index and neck circumference. Height was measured using a measuring tape by making the subject stand and was measured in centimetres (cm). Weight of the subject was recorded in kilograms using the portable weighing machine. Body mass index (BMI) was calculated using the formula weight (in Kg)/height in metre2. Neck circumference was measured using a measuring tape around the neck in inches. Statistical analysis: All the data were expressed as mean ± standard error. The means were analyzed by one analysis of variance (ANOVA) with multiple comparison test of Student Newman Keuls test. Correlations were investigated by calculating Pearson’s correlation coefficient test. Statistical analysis as well as plotting graphs was carried out using Sigma Plot 13.0 (Systat software, USA). P < 0.05 was considered as significant. Ethical consideration: The present study was approved by institutional human ethical committee, Saveetha University - IHEC No-008/12/2014/IEC/SU, dated - December 18th, 2014, Chennai, Tamil Nadu. The study protocol was as per the guidelines of ICMR. Confidentiality of the data was maintained. RESULTS The value of anthropometric parameters such as height, weight, waist circumference and body mass index are compared between control, prediabetes and OSA given in figure1. Body Weight among participants was higher in the OSA. Body mass index was higher in OSA and prediabetic group with mean 31.79 and 28.08 compared to the subjects in the control group (24.72). An increase in the mean values of the neck circumference was also observed in the OSA group with 38.40 followed by the prediabetes group with 33.94 the control group with 29.63.In the anthropometric parameters, weight, BMI & neck circumference were significantly higher in prediabetic and OSA when compared to control group. Between prediabetic and OSA, the three values were significantly higher in the OSA group. Height was not a significant variable among all the three groups. Figure 1: Height, weight, body mass index (BMI) and neck circumference (NC) in control (C), pre-diabetic (PD) and obstructive sleep apnoea (OSA). Mean + SE (n = 50 each). The ‘F’ and ‘P’ values are by one way ANOVA. aSignificantly different from control bSignificantly different from pre-diabetic.
DISCUSSION The present study was undertaken to compare the anthropometric parameters in individuals with pre-diabetes and obstructive sleeps apnoea. Body Weight among participants was higher in the OSA. Body mass index was higher in OSA and prediabetic group with mean 31.79 and 28.08 compared to the subjects in the control group (24.72). An increase in the mean values of the neck circumference was also observed in the OSA group with 38.40 followed by the prediabetes group with 33.94 the control group with 29.63.In the anthropometric parameters, weight, BMI & neck circumference were significantly higher in prediabetic and OSA when compared to control group. Between prediabetic and OSA, the three values were significantly higher in the OSA group. Height was not a significant variable among all the three groups. The anthropometric profile of prediabetic and obstructive sleep apnea when compared with control reveal that prediabetic and OSA subjects show an increased body mass index along with an increased neck circumference. A study by Youssef et al reported class 3 obesity with mean BMI being 42.82 in subjects with OSA.6Reports from another study revealed that 70% of subjects with OSAS are overweight. An increased body weight could be a major risk factor for snoring and sleep apnea.7 Obesity is accountable for a pre-diabetic state and a predisposition to OSA.OSA subjects reported insulin resistance with elevated levels of glucose confirmed by fasting glucose, oral glucose tolerance test, and increase in fasting insulin and HbA1C levels.8 Impaired fasting insulin shows that the secretion of insulin from the beta-cells is affected. Intermittent hypoxia and re-oxygenation during OSA display an elevated reactive oxygen species (ROS). Since β-cells are sensitive to ROS, impairment in the functioning of β-cell may be observed. Severity in the impairment in β-cell increases with the severity of OSA and eventually leads to type 2diabetes.9 Obesity is considered a health disaster in both developed and developing countries. Even in developing countries like India and other Asian countries, the incidence of obesity is high and its co–morbid conditions a major health problem (James et al, 2004). Obesity is associated with both pre-diabetes and OSA.10 Increase in neck circumference (NC) is also associated with obesity. In general, obesity assessed by the Body Mass Index (BMI), but in OSA, increase in NC is more predictive index. Upper airway anatomical factors are thought to play a critical role in the pathogenesis of airway closure in OSA and the risk of OSA tends to increase with obesity and increasing neck size.11,12Several factors contribute to reduction in airway calibre especially in the pharyngeal region in people with OSA. General factors are enlargement of soft tissue in this region and fat deposition and genetic factors which influence the bony structure. During sleep, pharyngeal dilator muscle activity which normally keeps this part of the airway patent is reduced; further, there is decrease in muscle tone during REM sleep and influence of gravitational forces in the supine position (Harrison). Consequently, there is a tendency for airway collapse leading to hypoxia.13 The tendency to airway collapse increases with obesity and increasing neck size (Davies et al, 1992) Diagnosis of OSA is currently based on a combination of clinical features and overnight polysomnography (PSG) which is expensive, time consuming and requires subjects to sleep overnight in a laboratory.14,15 A simple predictor for OSA is neck circumference (NC) rather than BMI.
CONCLUSION The study results support the importance and value of the anthropometric parameters in the pre-diabetes and obstructive sleep apnea conditions. Further detailed studies with higher sample size and multi center studies are recommended in this area for better understanding the relationship between these parameters, which helps to design effective treatment modalities.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.