 Home
Home
|
Table of Content - Volume 15 Issue 3 - September 2020
Sayed Badar Daimi1, Khuteeja Ruhi2, Mohammad Suhail3*, Afshan Kausar4
1,3Associate Professor, 2Faculty, Apex Medical Academy, 4Assistant Professor, Indian Institute of Medical Science and Research, Warudi, Tq Badnapur, District- Jalna, Maharashtra 431202, INDIA. Email: albadar085@gmail.com
Abstract Background: Childhood obesity is a serious medical condition that affects children and adolescents. Childhood obesity is particularly troubling because the extra pounds often start children on the path to health problems that were once considered adult problems - diabetes, high blood pressure. Aims and Objectives: In the present study we have investigated the prevalence of obesity and overweight and their association with the risk factors like diet, physical activity, sedentary lifestyle, eating habits, family history of diabetes and obesity. Material and Methods: Children between 6 and 15 years were sampled using multistage random sampling with population size of 250. Anthropometric data was analyzed using WHO charts for BMI in boys and girls of 2 to 19 years. The obesity and overweight were considered using an updated WHO based body mass index (BMI) reference. The association of physical activities, sport, sleeping habit, eating habits and family history of high blood pressure, obesity and diabetes with childhood obesity by a predesigned and pretested interviewer administered questionnaire was used to collect information. Results: Prevalence of underweight, healthyweight and overweight+obese was found to be 28%,44% and 28% among boys and 20%, 37%, and 43% among girls respectively. Eating habit like junk food, chocolate, eating outside at weekend and physical activity like exercise, sports, sleeping habit in afternoon showed remarkable effect on prevalence on overweight and obesity. Family history of diabetes and obesity were also found to be positively associated. Conclusion: The study concludes that, healthy eating habits in the form of fruits and vegetables in diet regularly and avoiding junk and restaurant food helps in maintaining ideal healthy weight and BMI. It is also found that having adequate physical activity in the form of participation in sports and exercise regularly at the same time avoiding excessive sleep have beneficial effects in enjoying healthy life. Key Words: childhood obesity, BMI, Physical activity, eating habits.
INTRODUCTION Obesity is a condition of excess body fat often associated with a large number of debilitating and life-threatening disorders.4 The problem is global and is steadily affecting many low- and middle-income countries, particularly in urban settings. The prevalence has increased at an alarming rate. Childhood obesity is one of the most serious public health challenges of the 21st century. Globally, in 2016 the number of overweight children under the age of five, is estimated to be over 41 million.1 The proportion of children in the general population who are overweight and obese has doubled over the past two decades in developed and developing countries including India.2Many studies have shown that the prevalence of overweight among adolescents varies between 10 and 30%. Childhood obesity is associated with various health-related consequences. Obese children and adolescents may experience immediate health consequences and may be at risk for weight-related health problems in adulthood. Being overweight or obese at a young age is linked to several health and economic consequences and it is therefore important to study the causes and risk factors and identify the best prevention and treatment strategies. Childhood obesity is a multifactorial condition, so it is important to be tackled at multiple levels, including individual, household, institutional, and community. This study will help us to understand the potential causes and risks associated with childhood obesity. Finally, there is a focus on ways to prevent childhood obesity as prevention strategies are key to reducing the epidemic. The present study has been conducted to estimate the prevalence and determinants of overweight and obesity among school children aged between 6 and 15 years, in city of Aurangabad, Maharashtra state.
MATERIALS AND METHODS Study Design: This was a school-based, cross-sectional, questionnaire based study carried out over a period of three months, from July to September 2018. We adopted a multistage stratified random sampling procedure. For the selection of schools, a list of all schools was obtained. Six schools were selected by a simple random technique. Selection of subjects: (inclusion and exclusion of students) Subjects were children, 6 to 15 years of age, in the city of Aurangabad, Maharashtra. After reaching the concerned school, the classes were selected randomly from each grade. Students were selected from each class by the simple random technique, using the students register, till the desired sample from each class was met. From each institution, at least 50 subjects were recruited. If a designated student could not be contacted or was not cooperative during the three separate visits, the subject was considered as a non-respondent. Children with history of chronic diseases like Tuberculosis, asthma, diabetes were not included. Anthropometric measurements: Trained investigators weighed all of children without shoes and heavy clothing, using an electronic weighing scale with an error of ±100 g. The weighing scale was regularly checked with known standard weights. A portable anthropometric rod was used for measuring the height, with an error to the nearest of 0.1 cm, using standard procedures. Questionnaire: A predesigned and pretested interviewer administered questionnaire was used to collect information. Information was collected on physical activity, such as participation in sports and games, aerobic physical exercises. Diet preferences for chocolate, biscuits, chips, and colas were taken into consideration. Trained interviewers administered the questionnaire to all children who attended school on the day of the survey. Students were asked to bring the completely filled questionnaire by their parents next day. Children who were absent from school because of sickness or other reasons were not followed-up. Statistical Analysis: Body mass index (BMI, kg/m2) was calculated on measured height and weight and was used to identify underweight, overweight and obese conditions using age and sex appropriate normative cut points. For classification, WHO reference charts for BMI, 2007 different for boys and girls, was used. Children were categorized into three groups namely underweight (≤ 5th percentile), normal (5th to 85th percentile) and overweight (≥ eighty-fifth percentile) + obese (≥ ninety-fifth percentile). We examined the prevalence of overweight, healthy weight and underweight in each gender by age group and sex. Group comparisons were performed using pie diagrams gender wise (Boys and Girls) Percentage of subjects from each category of underweight, healthy weight and overweight obese was calculated for each question like
The result for questionnaire based factors were represented in the form of bar diagram. Analysis was done depending upon the percentage of subjects in each category for each factor.
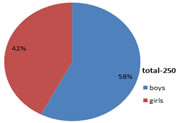
OBSERVATIONS AND RESULTS A total of 250 children in the age group of 6 to 15 years were analyzed. Out of these 144 (57.6%) subjects were males and 106 (42.4%) subjects were females.
Figure 1: Genderwise distribution of subjects
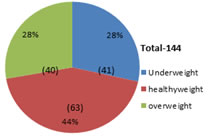
Body Mass Index We have categorized boys and girls as Underweight (UW), Healthy weight (HW) and Overweight + Obese (OW). The average Body Mass Index (BMI) for boys was 18.6 and that of girls was 19.09.
Figure 2: BMI category for Boys
In boy’s category, 41 (28.47%) were underweight, 63 (43.75%) were healthy weight and 40 (27.7%) were Overweight + Obese
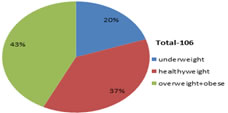
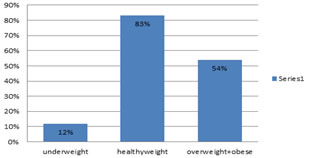
Figure 3: BMI category for Girls
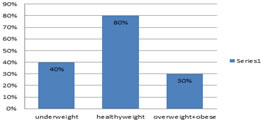
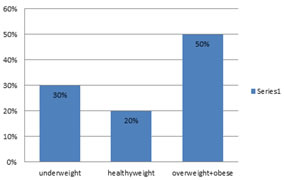
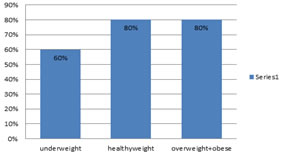
In girl’s category, 19 (17.92%) were underweight, 36 (33.96%) were healthy weight and 51(48.11%) were Overweight + Obese Figure 4: Participation in sports (boys)
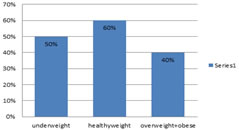
Figure 5: Participation in sports (Girls)
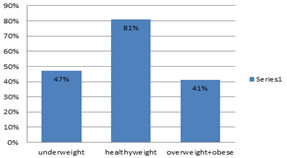
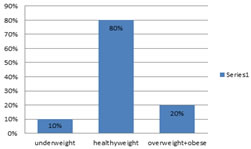
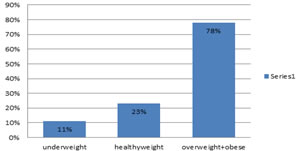
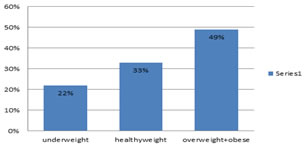
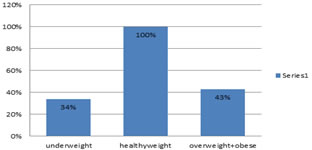
From the above Bar Diagram it has been found that, more no. of subjects participating in sports are from healthy weight group whereas less no . of subjects participating in sports belonged to underweight and overweight + obese. Thus participation in sports helps in maintaining healthy weight and prevents obesity and underweight. Figure 6: Physical exercise ( Boys)
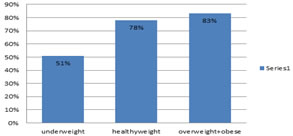
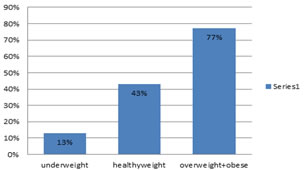
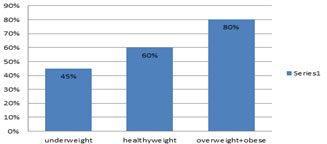
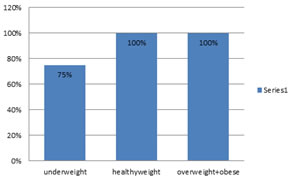
Figure 7: Physical exercise (Girls) From the above Bar Diagram it has been found that, more no. of subjects doing physical exercise are from healthy weight group whereas less no . of subjects doing physical exercise belonged to underweight and overweight + obese. Thus physical exercise helps in maintaining healthy weight and prevents obesity and underweight.
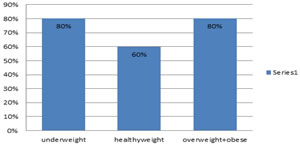
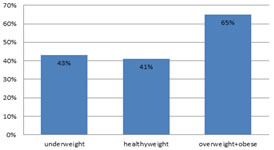
Figure 8: Sleeping habit in afternoon (Boys)
Figure 9: sleeping habit in afternoon (Girls) From the above Bar Diagram it has been found that, more no. of subjects have sleeping habit in afternoon who belonged to overweight + obese, whereas less no . of subjects have sleeping habit in afternoon who belonged to healthy weight group.. Thus sleeping habit in afternoon may be one of the factors for obesity and underweight.
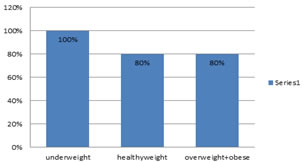
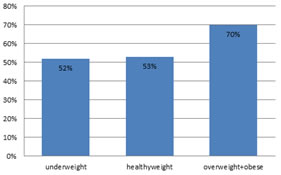
Figure 10: Restaurant visit per week (Boys)
Figure 11: Restaurant visit per week (girls)
From the above Bar Diagram it has been found that, more no. of subjects from overweight and obese group frequently visited restaurants,whereas less no . of subjects visited restaurants from underweight group and healthy groups. Thus subjects from overweight and obese ate food from outside regularly , hence this can also be one of the factors for obesity.
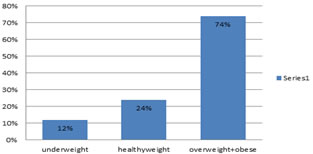
Figure 12: Taking junk food regularly (Boys)
Figure 13: Taking junk food regularly ( Girls)
From the above Bar Diagram it has been found that, more no. of subjects from overweight + obese group took junk food on regular basis whereas very less no . of subjects from healthy weight group and less no. of subjects from underweight groups took junk food regularly . Thus junk food might be one of the reasons for obesity.
Figure 14: chocolate eating habits (Boys)
Figure 15: chocolate eating habits (Girls)
From the above Bar Diagram it has been found that, subjects from overweight and obese have the habit of eating chocolate at its maximum level which is shown almost similar with the result of underweight and healthy weight groups. Thus results shows that chocolate eating habit has no significant effect on obesity.
Figure 16: Family history of Diabets (Boys)
Figure 17: Family history of Diabetes ( girls)
From the above Bar Diagram it has been found that, maximum subjects from all groups have a family history of diabetes. Thus family history of diabetes might not be factor of obesity.
Figure 18: Family history of Obesity ( Boys)
Figure 19: Family history of Obesity ( Girls)
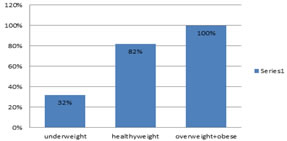
From the above Bar Diagram it has been found that, more no. of subjects from Overweight+obese group have a family history of obesity when compared to the subjects of underweight and healthy weight subjects. Thus family history of obesity is a very strong factor for obesity.
Figure 20: Family history of Hypertension (Boys)
Figure 21: Family history of Hypertension (Girls)
From the above Bar Diagram it has been found that, more no. of subjects from overweight + obese(girls) had a family history of hypertension whereas in boys many subjects have a family history of hypertension. Thus both in boys and girls there is good percentage of obese subjects with family history of hypertension .
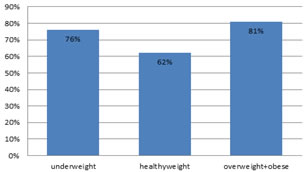
Figure 22: Fruits eating habit (Boys)
Figure 23: Fruits eating habit (Girls)
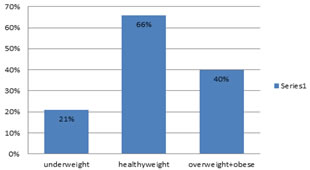
From the above Bar Diagram it has been found that, subjects with healthy weight have a very good habit o eating fruits which is less in no. when compared to subjects in the groups of underweight and overweight + obese. It can be a prevention method to eat fruits.
Figure 24: Vegetables eating habits (Boys)
Figure 25: Vegetables eating habits (Girls)
From the above Bar Diagram it has been found that, subjects from healthy weight group have a good habit of eating lot of vegetables which is found to be very less in underweight group subjects and good in overweight and obese subjects.
A total of 250 children in the age group of 6 to 15 years were analyzed. Out of these 144 (57.6%) subjects were males and 106 (42.4%) subjects were females. We have categorized boys and girls as Underweight (UW), Healthy weight (HW) and Overweight + Obese (OW). The average Body Mass Index (BMI) for boys was 18.6 and that of girls was 19.09. In boy’s category, 41 (28.47%) were underweight, 63 (43.75%) were healthy weight and 40 (27.7%) were Overweight + Obese. In girl’s category, 19 (17.92%) were underweight, 36 (33.96%) were healthy weight and 51(48.11%) were Overweight Obese. Overall, the study demonstrated that, sedentary behavior and physical activity in children influenced prevalence of overweight and obesity. In the present study, we found that junk food and chocolate eating habit have positive relation with prevalence of obesity and overweight. In the present study, we found that family history of obesity was more likely to have more prevalence of obesity and overweight than those having family history of diabetes. It was also found that eating habits of fruits and green leafy vegetables was high in healthy weight subjects and low in both, underweight and overweight subjects.
DISCUSSION There are wide spread reports regarding the trend of increasing prevalence of overweight and obesity among children and adolescents. The estimated prevalence of overweight among US children in 1999-2000 was more than 15%, and the value in Australia was almost 20%. In Brazil, the prevalence of overweight among school children has tripled and increased from 4% in the 1970s to 14% in late 1990s. In Egypt 14% of children were overweight or obese in 1997. However, recent studies in India and other countries revealed that obesity is becoming a growing health problem among children and adolescents, especially in urban populations.2 Sedentary behavior and physical activity in children may be predictive of body mass Index in adulthood. Sleeping habit in afternoon, decreased sports and exercise have also been implicated in childhood obesity because they reduce resting metabolism results in reduction of physical activity. A change in the amount of daily physical activity may account for improper balance between energy intake and energy expenditure. In the present study, physical activity in childhood attenuated BMI and these findings are consistent with studies that showed that body mass in children is influenced by the sleeping habit in afternoon, lack of physical exercise, and sports habit because sleeping habit in afternoon influenced BMI through displacing the time that could be utilized playing sports or engaging in other forms of physical activity. Reduced levels of physical activity may also lead to lower energy expenditure, thus affecting resting metabolic rate and total energy expenditure. In our study, we found that obesity and overweight have inverse relationship with physical activity. These data are consistent with previous studies in different countries.6 These data suggest that decrease in physical activity are due to expending less energy in activities of daily living, and at work. Thus, an active lifestyle during childhood can play an important role in optimizing growth and development during entire life. We recommend Comprehensive school and community programs to be developed to promote physical activity among children. Questionnaires about frequency of visiting restaurants per week and habit of having junk food provide information about subsequent health outcomes. Such information in various studies in children permits individual diets to be related to subsequent health outcomes.7 We focused our analysis on junk food and chocolate eating habits and frequency of restaurant visit per week because that they have special roles in obesity. In the present study, we found that junk food and chocolate eating habit have positive relation with prevalence of obesity and overweight. Eating all kinds of green leafy vegetables can be a step towards prevention and to avoid obesity and to be healthy. These results correlate well with previous reports which suggest that junk food (bakery items, pizza, burger, cheese, butter, oily items) chocolate intake tends to be more common among overweight and obese adolescents than among normal-weight adolescents. Junk food contains more amount of fat than carbohydrate and protein. Fat is less satiating than carbohydrate and dietary fat is stored more efficiently than carbohydrate or protein which finally results in obesity or overweight. Similarly, irregular food intake deleteriously affects nutritional health, reduces energy levels and promotes the consumption of high caloric food later in the day.2 Provisions of healthy foods options and physical activities for children and adolescents are need of hour of public health initiatives to curb an obesity pandemic. Thus, our data showed effects of sedentary behavior and physical activity on prevalence of underweight, overweight and obesity. Prevalence of overweight and obesity are more in children with family history of diabetes and obesity. 8 In the present study we found that family history of obesity was more likely to have more prevalence of obesity and overweight than those having family history of diabetes. Our results correlate with previous study which suggest that family history of obesity have more prevalence to obesity than family history of diabetes. This indicates that children having family history of obesity are more likely to become obese or over weight. Overall, the study demonstrated that, sedentary behavior and physical activity in children influenced prevalence of overweight and obesity. Prevention of obesity in children is easier than the adults. Based on the findings of this study it is recommended that consumption of high fat and high energy food (Junk foods) and visiting restaurants more than once in a week should be avoided by children. Choosing healthy foods for infants and young children is critical because food preferences are established in early life. Feeding infants energy-dense, high-fat, high-sugar and high-salt foods is a key contributor to childhood obesity. Lack of information about sound approaches to nutrition and poor availability and affordability of healthy foods contribute to the problem. The aggressive marketing of energy-dense foods and beverages to children and families further exacerbate it. In some societies, longstanding cultural norms (such as the widespread belief that a fat baby is a healthy baby) may encourage families to over-feed their children.1 The increasingly urbanized and digitalized world offers fewer opportunities for physical activity through healthy play. Being overweight or obese further reduces children’s opportunities to participate in group physical activities. They then become even less physically active, which makes them likely to become more overweight over time.1 Sedentary life style should be discouraged. Increase physical activity like playing outdoor games, walking, cycling should be encouraged in children. Health education should be given to parents, teachers and children regarding dietary habit and sedentary life style (school based intervention).
CONCLUSION Childhood obesity is a problem of great concern and actions needs to be taken to curb it. From this study we conclude that, healthy eating habits in the form of fruits and vegetables in diet regularly and avoiding junk and restaurant food helps in maintaining ideal healthy weight and Body Mass Index. It is also found that having adequate physical activity in the form of participation in sports and exercise regularly at the same time avoiding excessive sleep have beneficial effects in enjoying healthy life. We recommend health education should be given to parents, teachers and children regarding dietary habits and sedentary life style and schools are best place to implement these (school based intervention).Sedentary life style should be discouraged. Increase physical activity like playing outdoor games, walking, cycling should be encouraged in children. These small but important Public health interventions at the individual and policy-making levels need to be instigated at the earliest to tackle the problem of childhood obesity. Healthy habits should be inculcated, beginning from childhood for all but specifically to children with family history of obesity, diabetes and hypertension. This will help us to build healthy and productive future generation, in turn healthy society and healthy-progressive INDIA as a whole.
ACKNOWLEDGEMENT I acknowledge the support of management and Dean of Indian Institute of Medical science and research, Badnapur for providing all logistics for research. REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.