 Home
Home
|
Table of Content - Volume 20 Issue 3 - December 2021
Effect of body mass index on heart rate recovery following treadmill exercise in healthy aircrew
Udaya IB#, Laxmi CC†, Akhilesh Goyal$, Polash Sannigrahi*
#Aerospace Medicine Specialist, $Medicine Specialist, *Aerospace Medicine Specialist, Institute of Aerospace Medicine, Bengaluru, INDIA. † Associate Professor, Department of Physiology, FIMS, Kadapa, INDIA. Email: laxmicariappa@gmail.com
Abstract Background: Increased adiposity results in an altered autonomic nervous system. Autonomic dysfunction can be assessed by heart rate recovery (HRR) following graded exercise. HRR is an indicator of cardiac autonomic function. Aims and objective: To study the effect of body mass index (BMI) on heart rate recovery following treadmill exercise in healthy aircrew. Materials and Methods: In this cross-sectional study, 30 aircrew in the age group 30 to 50 years were selected. The BMI of the participants were calculated. HRR was assessed during the recovery period following the treadmill stress test. Heart rate recovery (HRR) was obtained by computing the difference between heart rate at the end of exercise and 1 min heart rate post-exercise during recovery. Result: There was a negative correlation between BMI and HRR1 (r= -0.354 p=0.04). Conclusion: There was a negative correlation between BMI and HRR in aircrew. An increase in BMI has a tendency to slow HRR due to decreased parasympathetic activity. Losing weight will help to improve HRR and thus reduce the risk of cardiovascular diseases. Keywords: Body mass index, heart rate recovery, parasympathetic reactivation.
INTRODUCTION The prevalence of the cardiovascular disease is high among overweight and obese individuals. This is due to altered cardiac autonomic regulation.1 Obesity results in decreased parasympathetic activity and increased sympathetic activity.2 The cardiac autonomic function can be assessed by heart rate recovery (HRR) following exercise like the treadmill test.3 Heart rate recovery is defined as the rate at which heart rate decreases following exercise which is due to reactivation of parasympathetic system and withdrawal of sympathetic system. Heart rate recovery is a non-invasive test which gives information regarding vagal control. HRR is measured as the difference between peak heart rate at the end of exercise and heart rate in 1 min during recovery following a graded treadmill exercise. If the HRR in 1 min is < 12 bpm, it is considered as a slow recovery of the heart rate which is due to impaired parasympathetic system reactivation. Attenuated HRR is an independent predictor for cardiovascular and all-cause mortality.4,5,6 HRR has shown to be inversely related to insulin resistance, hyperlipidaemia, and metabolic syndrome.7 Previous studies have reported that there is a negative correlation between obesity and heart rate recovery.8 There is a slow HRR in overweight and obese individuals compared to normal-weight individuals.9 It is also seen that obese individuals have high resting heart rate and low peak heart rate during exercise.10 HRR improves after weight loss in overweight and obese individuals.11 Obesity is one of the major risk factors for cardiovascular diseases. Body Mass Index (BMI) is used as one of the criteria to determine the overweight and obese status of an individual.12 Impaired HRR is associated with higher BMI which could be due to vagus nerve dysfunction. Aircrew are exposed to various stressors. The recovery phase after exercise is a vulnerable phase for various cardiovascular events such as sudden cardiac deaths. Prevention is the mainstay in aviation medicine. Autonomic evaluation in terms of Heart rate recovery can be used to assess parasympathetic reactivation following exercise in aircrew. So this study is designed to assess heart rate recovery following treadmill exercise in aircrew and to find the correlation between BMI and HRR in healthy aircrew.
MATERIAL AND METHODS General Study Design: 30 healthy male aircrew in the age group of 30-50 years participated in this cross-sectional study. Aircrew with diabetes mellitus, hypertension, other cardiovascular diseases, renal diseases, endocrine disorders, CNS disorders, anemia, lung disorders or having a physical disability which affects walking, e.g. arthritis of the knee or hip, amputations, etc. were excluded from the study. All exercise testing were performed at the Department of Physiology, Institute of Aerospace Medicine, Bangalore. Exercise Tests were carried out between 9 AM to 11 AM, in a quiet room. The participants were asked to fill a questionnaire to assess their physical activity status. A brief history, general and systemic examination were performed. The experimental protocol was fully explained to the participants to allay apprehension. They refrained from any energetic physical activity for 2 to 3 hours before the test. Informed consent was taken from all the subjects. The study was approved by the institutional Ethical Committee. Estimation of Body Mass Index: The weight of the participants was measured using calibrated weighing machine in light clothing and bare feet. Their height was measured using the measuring scale in centimeters which was fixed to the wall. Body mass index was calculated using Quetelet's index i.e. BMI = Weight (kg) / height (m2). Estimation of HRR following treadmill test: The exercise test was conducted in a motorized Treadmill (Mortara X-Scribe manufactured by Mortara Instruments. inc,) using Bruce protocol. Each subject was familiarized initially with the instrument before performing exercise for the study. After adequate rest, subjects were made to walk/run as per ‘Bruce protocol’. Once the subjects achieved the MHR or if there were any endpoints the recovery mode was initiated. During recovery mode, the speed of the treadmill was reduced to 1.7 km/hr before complete stoppage. Heart rate was recorded at the end of exercise and 1 minute and 2 minutes after exercise (HRR1). HRR was obtained by computing the difference between heart rate at the end of exercise and 1 min heart rate post-exercise during recovery. HRR2 at the end of 2 mins was calculated. Statistical analysis: Obtained data were entered in Microsoft ® Office Excel ® 2013 Professional. All statistical analyses were performed using SPSS software (version 16.0, SPSS Inc., Chicago, Illinois). Pearson’s Correlation was used to find the correlation between BMI and HRR1and HRR2. A p-value of < 0.05 was considered to be statistically significant.
RESULTS Table 1: Correlation between BMI and HRR1 and HRR2
BMI- Body Mass Index, HRR1- Heart Rate Recovery in 1 minute, HRR2-heart rate recovery in 2 minutes. *p-value < 0.05.
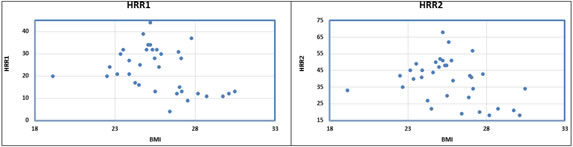
Figure 1: Pictorial representation of the correlation between; Figure 2: Pictorial representation of the correlation between BMI BMI and HRR1 and HRR2
A total of 30 male subjects participated in this study. Their mean age, height, and weight were 42 ± 5.20yrs, 1.73 ± 0.05 m, and 77.06 ± 7.16 kg respectively. The average BMI was calculated to be 25.01±2.22 kg/m2. There was a significant negative correlation between body mass index and heart rate recovery in 1 minute (r= -0.354 p=0.04). A significant negative correlation was also observed between body mass index and heart rate recovery in 2 minutes following exercise (r= -0.341 p=0.04).
DISCUSSION Slow heart rate recovery is an independent risk factor for cardiovascular and all-cause mortality. The prevalence of the cardiovascular disease is also high among overweight and obese individuals. Rapid heart rate recovery response to exercise is a marker of physical fitness and also has prognostic value. This study was done to know the effect of body mass index on heart rate recovery (parasympathetic reactivation) following treadmill exercise in healthy aircrew. There was a negative correlation between body mass index and heart rate recovery in 1 minute and 2 minutes following exercise. But clinically HRR in 1 minute is more significant because it represents parasympathetic reactivation following exercise test. Similar results were also observed by Dimpka et al. and they reported that BMI in men showed the strongest independent association with HRR.8 Arpita et al. in their study found abnormal heart rate recovery among obese individuals.13 This finding could be because of the altered autonomic nervous system function, specifically reduced parasympathetic activity in overweight and obese individuals. L Gondoni et al. compared HR behaviour in a trained and untrained obese individual with normal BMI individuals during exercise and concluded that obese individuals irrespective of fitness had slow HRR.14 Barbosa et al. in their study concluded that there is an association between obesity and impaired HRR after exercise which may be useful in the early identification of individuals at risk of cardiovascular events.9 Weight loss was associated with improved HRR indicating increased vagal tone.9 Weight loss altered autonomic balance by modulating parasympathetic activity.15 Anand A et al. in their study found a negative correlation between obesity indices and HRR but was not significant. This finding is contrary to other works which could be due to very young subjects (18 -30 yrs) being enrolled for the study.16 Obesity causes chronic inflammation which could result in altered autonomic functions.17 Obesity affects autonomic function by increasing renin-angiotensin activity. Baroreceptor sensitivity is also affected by excess body fat (18). Parasympathetic reactivation which normally occurs following exercise which brings the heart rate back to normal in the early phase following exercise is also affected. This could be due to vagus nerve dysfunction.
CONCLUSION There was a significant negative correlation between body mass index and heart rate recovery following exercise. This suggests that increased body mass index has the tendency to impair autonomic modulation. Weight loss will help in improving HRR and thus reduce the risk of cardiovascular diseases. Limitations: In our study sample size was small and only male participants were enrolled. Other obesity indices excluding BMI can be used to find the correlation between obesity and HRR. Acknowledgments: We thank all the participants who took part in this study.
REFERENCES
Policy for Articles with Open Access
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.