 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 7 Issue 2 - August 2018
25 hydroxy vitamin D status and cognitive impairment in the elderly among Indian population
Basheer M P1*, Pradeep Kumar K M2, Muneer R E3, Sreekumaran E4, Ramakrishna T4
1Al Azhar Medical College and Super Specialty Hospital Thodupuzha, Kerala, INDIA. 2Goverment Medical College Calicut, Kerala, INDIA. 3Physician, Co Operative Hospital Vatakara, Kerala, INDIA. 4Department of Life Sciences, University of Calicut, Kerala, INDIA. Email: drbasheermp@gmail.com
Abstract Background: Cognitive function is a major determinant of quality of life in older age. The number of elderly subjects who will suffer from cognitive impairment and dementia will further increase in the near future.Cognitive impairment can be influenced by a number of factors and the potential effect of nutrition has become a topic of increasing scientific and public interest.Vitamin D might contribute to age-associated cognitive impairment and dementia. The present study is designed to know the role of 25 hydroxy vitamin D and its relation with human cognition. Materials and Methods: A total of 337 subjects with a mean age of 49 participated in the cross sectional study from different parts of Kerala state in India. Participants were administered a series of neuropsychological test batteries with major emphasis on 7-minute screen test. All test procedures were administered by standard protocol after a written consent was obtained from the participating subjects. Analysis of 25 hydroxy vitamin D was done using serum samples and the data obtained was then statistically analyzed using SPSS software version 17. Results: 25 Hydroxy vitamin D was found to be significantly related to the cognitive score (P< 0.001). Conclusion: The results of our study gives us an insight that Vitamin D may be associated with cognitive function in elderly population. But further studies on a larger population is required to come out with a definite conclusion. Key Words: Cognition, Vitamin D, 25 Hydroxy Vitamin D and Dementia.
INTRODUCTION Vitamin D is a neurosteroid hormone which may regulate neurotransmission, neuroprotection and neuroimmuno-modulation. Vitamin D receptors have been located in the human cortex and hippocampus1, which are key areas for cognitive functioning and their absence has been associated with neurodegenerative dementia such as Alzheimer’s disease2. Low vitamin D status has previously been reported in patients with Alzheimer’s disease3, and that vitamin D is important for normal neural function is supported by the presence of vitamin D3 25-hydroxylase and 25-hydroxy vitamin D3-1α-hydroxylase in brain tissue4. A beneficial effect of vitamin D for cognition potentially could be mediated through a increasing acetylcholine concentration in the brain, as suggested by the finding that 1, 25- dihydroxy cholecalciferol – (1, 25-(OH)2 D3 /vitamin D3) treatment increases choline acetyltransferase activity in specific rat brain nuclei5. Another relatively direct effect could be through increased neurotrophin synthesis. Enhanced neuroprotection by vitamin D, as demonstrated in several models of neuro degeneration, could also contribute to maintaining normal cognitive function. Vitamin D could be valuable in the prevention and/or treatment of neurodegenerative diseases6.It is plausible that such neuroprotection could be mediated through a reduction of free radicals in brain tissue.There is evidence of neuroprotective functions of vitamin D and growing evidence of a potential role of vitamin D in cognitive function7. Vitamin D may help to prevent neurodegenerative diseases of aging through protection against co-morbidities such as cardiovascular and cerebro-vascular disease,8 peripheral artery disease9, oxidation and inflammation and neuronal health.In the elderly individuals, low 25 hydroxy vitamin D {25(OH) D} is associated with dementia; further associations between 25(OH) D and white matter hyper intensities (WMH) support the hypothesis that vascular factors may mediate the association between vitamin D deficiency and cognitive function. Buell et al.,10reported a significant association between 25(OH) D concentration and executive function and global cognition and they have identified associations between 25(OH) D concentrations and diagnoses of AD and stroke (with and without symptoms of dementia). WMH are also associated with brain atrophy, impaired cerebral vascular function and poorer frontal lobe cognition11. In contrast, one study of older adults (aged 60 years) in the third US National Health and Nutrition Examination Survey (NHANES III) reported an inverse association, with higher circulating 25(OH) D being associated with poorer cognitive function12.In another study, no significant difference was observed in levels of serum 25(OH) D when comparing 16 dementia cases and 16 controls13. Since thereare lot contracdiction regarding serum level of elcrtolytes, vitamin B complex and vitamin D on cogniveimpairment,wetries to explain the importance of 25, hydroxy vitamin D in cognitive performance in the elderly among Indian population based on 7 Minute screen test. Our previous studies poved that there is association of serum level of electrolytes and vitamin B complexes on cognitive impairment14,15 MATERIALS AND METHODS Study Participants: Participants were a part of cross-sectional study of Calicut University Project to Investigate Memory and Ageing (CUPTIMA), as adapted and standardized for Malayalam speaking population16. We administered a series of Neuropsychological test batteries to 337 healthy individuals belonging to various places of Kerala state in India, especially Trissur, Palakad, Malappuram and Kozhikode districts, for about a 7 year period. All of them except three were left handed and none of them were inarticulate. Only participants who were having no history of stroke, head trauma, neurological disease, psychological illness, or any other known present illness and those who know Malayalam or English or both were chosen as participants. Individual participants were subjected to different test batteries.Participants ranged from ages of 20 to 84 years with a mean age of 49, having educational backgrounds ranging from four to twenty years. Participants were grouped into categories based on their sex and age. All test procedures were explained and written consent was obtained from each. All the tests were administered based on standard protocol (Oxford Project to Investigate Memory and Ageing [OPTIMA], Cambridge examination of mental Disorders in the Elderly [CAMDEX] and CUPTIMA Methods: We had undertaken 7-minute screen test to know the cognitive impairment especially dementia prone Alzheimer’s disease.The scores obtained from all the above tests were then analysed using the scoring calculator, to find out the probability of dementia related problems17.Serum 25-Hydroxy vitamin D was assayed using Architect 25- OH Vitamin D i System (Abbott). Statistical Analysis: The data of biochemical test parameters was analyzed with SPSS software version 17. Statistical tests were conducted for analysis, which include ANOVA, Independent sample test and Pearson correlation.
RESULTS The 7- Minute screen test was administered in all the age groups and found an increasing trend in the score as age advanced (Table 1) A statistically significant difference was found between younger age group (20-29) and other groups (p<0.05. No statistically significant difference was observed between the scores of males and females (p=0.171).
Table 1:Mean 7-Minute screen test score in different age groups, education category and sex of participants.
Based on the 7 - minute screen test, probability of dementia in the different age groups was also calculated. The participants with 75.81 ± 6.92 age (n=43) showed high probability to dementia (HI) than the lower age group ‘LO’ (44.33 ± 16.56, n=286). A statistically significant difference in dementia probability was observed between the higher and lower age groups (p<0.001) (Table 2), of which eight subjects were re checked (RE). Among HI dementia probability with Alzheimer’s characteristics, 39.5 % were males and 60.5 % were females.
Table 2:Dementia probability in different age groups (descriptive)
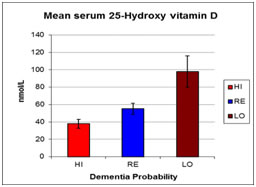
Serum vitamin D (25- Hydroxy vitamin D (25(OH) D) was estimated in all the selected participants based on dementia probablity. In the dementia probability LO group the mean serum Vitamin D was 97.938 ± 17.9336 and in the HI group it was 37.792 ± 5.0428. One way ANOVA was conducted between the groups and within the groups which showed a highly significant change. Between the groups, the mean square value was 11339.455 with a p value of <0.001 and within the groups the value was 141.500 with a p value of <0.001(figure 1).
Figure 1:Mean serum level of Vitamin D in different categories of participant groups Out of these selected participants for vitamin D estimation, 37.5% belonged to HI group, 37.5% belonged to LO group and remaining 25% belonged to RE group based on the 7- minute screen test. All the participants were well matched for age and sex. Descriptive statistics for 25 hydroxy vitamin D is presented in Table 3. A number of cognitive assessment tests were used to evaluate cognitive function in this population and a composite score was created to represent cognitive function/impairment. Table 3:Mean serum Vitamin D (25 (OH) D) values (nmol/L) in different categories.
DISCUSSION A number of small clinical studies suggest that serum 25-hydroxy vitamin D [25(OH) D] concentration, an effective indicator of vitamin D status, may be associated with poor cognitive function or dementia18.Similarly, a monotonic decrease in serum 25(OH) D was observed when patients with severe Alzheimer’s disease and mild AD cases were compared with controls19.It has been suggested that higher circulating levels of vitamin D improve cognitive function and studies in middle- and older-aged adults have shown positive associations between serum levels of 25-hydroxy vitamin D [25(OH) D] and cognitive functions20,21. Some earlier studies have suggested that vitamin D supplementation may exert a beneficial effect on cognitive function among older adults, because vitamin D binds to neural receptors in the brain thereby acting towards neuroprotection with its anti-inflammatory and antioxidative effects. Other related research has shown an association between vitamin D deficiency and dementia, particularly Alzheimer’s disease, suggesting vitamin D deficiency to be a measurable and modifiable risk factor for potential cognitive decline22.There is evidence to suggest that serum 25(OH) D is related to cognitive impairment in the elderly population and a potential diagnostic aid for screening or differential diagnosis. This is important because serum 25(OH) D may play an important role in the expression of neurotrophic factors, the stimulation of adult neurogenesis, calcium homeostasis, and detoxification23. Vitamin D contributes to neuroprotection by modulating the production of nerve growth, neurotrophin, glial cell derived neurotrophic factor, nitric oxide synthase and choline acetyl transferase24, and neuroprotective mechanisms including vasoprotection and amyloid phagocytosis and clearance25,26.Furthermore, the association between serum 25(OH) D levels and cognitive impairment underlines the importance of micronutrients in the elderly population. In another study, Llewellyn et al.,27observed that levels of serum 25(OH) D were generally lower in the cognitively impaired general population, and there was evidence for a monotonic relationship. Low levels of vitamin D were associated with substantial cognitive decline in the elderly population studied over a 6-year period, which rises important new possibilities for treatment and prevention28. Thus, our results also suggest that high levels of serum 25(OH) D are associated with lower odds of cognitive impairment.
CONCLUSION The results of our study give us an insight that 25 Hydroxy vitamin D may be associated with cognitive function in elderly population of our state Kerala in India. But further studies on a larger population is required to come out with a definite conclusion.
REFERENCES
|
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.