 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 7 Issue 3- September 2018
Effect of hypomagnesaemia on glucose homeostasis in diabetic foot ulcers
M Vijayamalathi*, P Kathiravan**, T S Ranjitham***, S Vadivel****
{*Assistant Professor, ****Professor and HOD, Department of Physiology} {**Sr. Resident, Department of Orthopedics} {***Assistant Professor, Department of General Surgery} Karpaga Vinayaga Institute of Medical Sciences, Madhuranthagam, Tamil Nadu. Email: pandu.kathir@gmail.com
Abstract Diabetes mellitus, a metabolic disorder has got complications like neuropathy, nephropathy, retinopathy, microvascular angiopathy and foot complications. Foot complications like foot ulcer, gangrene may end in amputation. Recent studies have stressed the role of hypomagnesemia as one of the contributing factors of diabetic complications. Our study was done to assess the level of serum magnesium level in subjects with diabetic foot ulcers to diabetics without foot ulcer and non-diabetic subjects. Totally 146 subjects were recruited in this study and were divided into three groups, namely, non-diabetics (group-I), diabetes without foot ulcer (group-II) and diabetes with foot ulcer (group-III). These subjects were investigated for FBS, HbA1c and serum magnesium. Analysis of the results obtained showed more pronounced hypomagnesemia in group-III than the other two groups and was statistically significant. Hence we conclude that level of serum magnesium plays an important role in diabetic foot ulcers. Key Words: Diabetes mellitus, Hypomagnesemia, foot ulcer.
Magnesium, a trace element, is one of the abundant cations in the body which plays a fundamental role in many enzymatic reactions and functions of the cell which includes energy metabolism and synthesis of protein.1 It is also a cofactor in synthesis of a major antioxidant, Glutathione. Glucose homeostasis reflects a balance between hepatic glucose production and peripheral glucose uptake and utilization. Insulin is the most important regulator of this equilibrium. Diabetes mellitus is a common metabolic disorder and its complications have become a threat in developing countries like India. Poor glycemic control leads to complications like microangiopathy, peripheral neuropathy and nephropathy. There is a direct relationship between complications of diabetes mellitus and chronic hyperglycemia.2 In our study we have focused on one of the morbid complications namely foot ulcers in diabetes. The aetiopathogenesis of foot ulcer is multifactorial and the major contributing factors are peripheral neuropathy and ischemia resulting from peripheral vascular diasease.3 Pathophysiology of impaired glycemic control is due to decreased insulin sensitivity and increased insulin resistance. Studies have shown that magnesium is necessary for synthesis and effective action of insulin. Hypomagnesaemia affects activation of tyrosine kinase in the receptors which leads to Insulin resistance.4 Our study was designed to evaluate the effect of hypomagnesemia in diabetic foot ulcers and will be compared with other two groups, namely non diabetic group and diabetic group without foot ulcers, as magnesium plays a major role in glycemic control.
MATERIAL AND METHODS This study was conducted in Karpaga Vinayaga Institute of Medical Sciences and Research Centre after getting the approval of institutional ethical committee and the written informed consent of the volunteers. Totally146 subjects were recruited in this study. The test group consisted of 49 patients with type 2 Diabetes mellitus without foot ulcer attending/admitted in wards of our Medicine department and 47 patients with type 2 Diabetes mellitus with foot ulcer attending/admitted in wards in our Surgical/Medicine department. The control group consisted of 50 volunteers with age and gender matched who are non-diabetic, apparently healthy subjects. Subjects with acute or chronic diarrhoea, hypertension, malabsorption, thyroid or adrenal dysfunction, history of chronic alcohol intake, taking drugs which are known to affect magnesium levels, pregnancy, lactation, chronic kidney disease and sepsis were excluded from this study. Primary data was collected by the investigators by structured questionnaire. Fasting venous blood samples were collected for estimation of Fasting blood sugar, HbA1c and serum magnesium levels. Diagnosis of diabetic foot ulcer was established by the presence of foot ulcerations with full-thickness skin defects, whose recovery time was longer than 14 days.5
RESULTS Out of 146 subjects recruited for this study, 49 were diabetic patients without foot ulcer, 47 were diabetic patients with foot ulcer and 50 volunteers with age and gender matched who are non-diabetic, apparently healthy subjects. The data obtained was entered in excel and analysed using SPSS software. The significance of the study parameters between three groups of the subjects was done by analysis of variance (ANOVA). Chi-square/Fisher Exact test was used to find the significance on categorical scale between two or more variables.
Table 1: Comparison of mean levels FBS, HbA1c and Serum Mg in three groups studied
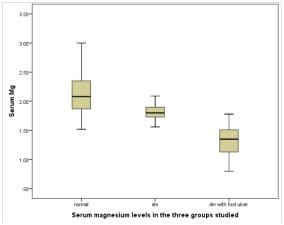
Table 2: Serum Magnesium levels in three groups studied
Lower levels of Serum Mg is significantly is associated with DM patients with P value
Figure 1
DISCUSSSION Diabetic mellitus is a symptom complex of an altered metabolic regulation and it causes secondary pathophysiologial changes in multiple organ systems which imposes tremendous burden on the individual with diabetes and on the health care system. Diabetes and its complications produce a wide range of symptoms and signs. It is the most common known metabolic disorder contributing to increased rate of wound infection and foot is a frequent site of complications in patients with diabetes. Once an ulcer has developed there is an increased risk of wound progression which may eventually lead to amputation. 40% of amputation is preventable by well regulated glycemic control. Hence, achieving optimal glycemic control should be the goal of any diabetic treatment protocol. In our study the mean fasting blood glucose level was 99.8±12.1, 153.2±11.03, 220.7±29.1 in non-diabetic (Group-I), diabetes without foot ulcer (Group-II) and diabetes with foot ulcer (Group-III) respectively. The mean HbA1c% was 5.26±0.66, 8.51±1.23, 10.4±2.02 in Group-I, II and III respectively. As per many studies4,5 magnesium deficiency is associated with insulin resistance and this induces or worsens the existing diabetes mellitus. The mean magnesium level in our study was 2.14±0.37, 1.81±0.12, 1.33±0.23 in Group-I, Group-II and Group-III respectively. A study by Fernando et al6 Mg deficiency may result in disorders of tyrosine kinase activity on insulin receptor and increased intracellular Calcium concentration which eventually leads to development of insulin resistance. Vijayalakshmi S et al7 explained in detail about the probable mechanism involved for the low levels of serum magnesium in diabetes. It is explained that, a two way process may be present in the pathophysiology of diabetes mellitus and its complications may be associated with hypomagnesemia. In diabetic subjects when the blood glucose level rises above the renal threshold, excretion of glucose in urine takes place and as a result of this osmotic dieresis, magnesium is also lost in urine leading to hypomagnesemia which may in turn worsen the diabetic status by altering the insulin secretion further. In our study hypomagnesaemia was more evident in the group of diabetes mellitus with foot ulcer than in the group of diabetes mellitus without foot ulcer. This is supported in a study done by Arudhati et al which says that statistically significant association was found only in association of foot ulcers and hypomagnesemia and not in other complications like diabetic retinopathy and nephropathy. Another study by Ankush et al1 stating that Mg deficiency has been proposed as a novel factor implicated in the pathogenesis of late complications of diabetes mellitus. HbA1c levels in our study were higher and Magnesium levels were lower in subjects having type2 diabetes mellitus than the non-diabetic subjects and this negative correlation between HbA1c and magnesium levels were seen in many studies2,3 The serum magnesium levels were significantly lower in diabetic subjects with foot ulcer than in the diabetic subjects without the foot ulcer which is in accordance with the study done by Sakir Ozqur Keshek et al5.
CONCLUSION In our study the level of serum magnesium in three groups were compared and was found that it was lower in subjects of diabetes mellitus with foot ulcer (Group-III)than the other two groups namely non-diabetic and diabetes without foot ulcer. The results were subjected to statistical analysis and were found to be statistically significant. Hence we conclude that glycemic control is mandatory to prevent foot ulcer complications in diabetic subjects. Our results re-emphasize the role of magnesium in diabetic complications (foot ulcer)
LIMITATIONS The study has a lower sample size and in our questionnaire we have not emphasized on detailed diet pattern.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.