 Home
HomeOfficial Journals By StatPerson Publication
|
Table of Content - Volume 8 Issue 2 - November 2018
Evaluation of serum gammaglutamate transferase levels in type 2 diabetic patients with and without neuropathy
Divya R1, Ashok V2*, Abeetha S3
{1Assistant Professor, Department of Physiology} {2Assistant Professor, Department of Biochemistry} Karpagam Faculty of Medical Sciences and Research, Coimbatore, INDIA. 3Assistant Professor, Department of Physiology, ACS Medical college and Hospital, Chennai, INDIA. Email: dr.ashokmbbs1986@yahoo.com
Abstract Background: Diabetic neuropathy is one of the common complications of diabetes mellitus. The pathophysiology of diabetic neuropathy is complex and recent studies have suggested the use of serum gammaglutamyl transferase (GGT) as an early marker of oxidative stress. In this study we investigated whether serum GGT may be useful in predicting diabetic neuropathy. Objective: This study was undertaken to investigate whether serum GGT is a useful marker of oxidative stress in type 2 diabetic neuropathy. Methods: Our study included64 patients with type 2 diabetes who were evaluated for the presence of neuropathy using clinical neurologic examinations including nerve conduction velocity studies. We evaluated the association between serum GGT and the presence of diabetic neuropathy. Results: The serum GGT concentration was significantly elevated in type 2 diabetic patients with neuropathy compared to patients without neuropathy (P < 0.01). Serum GGT was independently related with Malondialdehyde (MDA) according to linear regression analysis (P< 0.01). Conclusion: This study shows that increased levels of serum GGT may have important clinical implications in the presence of neuropathy in patients with type 2 diabetes. Serum GGT is a useful marker of oxidative stress in patients with diabetic neuropathy. Key Words: Diabetes mellitus; Gammaglutamy ltransferase; Oxidative stress; neuropathy.
INTRODUCTION Diabetes mellitus is associated with various complications including: heart disease, stroke, retinopathy, kidney disease, and neuropathy. Diabetic peripheral polyneuropathy is one of the most common complication of diabetes, with 60-70% of diabetic patients reporting mild to severe forms of peripheral nerve dysfunction. Diabetic neuropathy is characterized by a number of neural symptoms including numbness, sensory loss, and stabbing or burning pain typically experienced in the hands and feet.1 The prevalence of diabetic peripheral neuropathy in Type 2 diabetic subjects in an Indian study was shown to be 13.2%. Early recognition of diabetic peripheral neuropathy is necessary to prevent and treat diabetic foot and consequently amputation. Clinical symptom assessment, neurological examination and nerve conduction studies are used for diagnosing and staging severity of diabetic neuropathy.2 Diabetic peripheral neuropathy is multifactorial in origin. Oxidative stress is one of the common causes for its origin.3 The free radicals produced by oxidative stress leads to oxidation of polyunsaturated fatty acids resulting in the formation of lipid peroxidation products such as malondialdehyde (MDA). MDA is measured in serum samples as a biomarker of oxidative stress and lipid peroxidation.4 Gamma glutamyl transferase (GGT) has shown to be one of the early markers of oxidative stress in otherwise healthy individuals.GGT is a membrane bound enzyme and its main physiological function is to make cysteine available for regeneration of intracellular glutathione and protect against ROS causing oxidative stress.5 In this study we investigate serum gamma glutamyl transferase concentrations in diabetic peripheral neuropathy patients.
AIM AND OBJECTIVES
MATERIALS AND METHODS This study was conducted in the Department of Physiology at Sri Manakula Vinayagar Medical College and Hospital, Pondicherry, in collaboration with the Department of General medicine. This was a hospital-based case control study. This study was approved by the Institutional Ethics committee, Sri Manakula Vinayagar medical college hospital. The sample size was 64 subjects aged 35-55 years and they were divided into two groups Inclusion Criteria Exclusion Criteria Sample collection: Three ml of whole blood was collected from the controls and the study group after getting the informed consent. Then the serum was separated after subjecting the collected blood to centrifugation at 2500 rpm for 5min. The serum was divided into aliquots and stored at -20ºC for further analysis. Estimation of serum gammaglutamyl transferase: Serum gammaglutamyl transferase was measured by a modified Szasz method using CobasMiras plus Automated Chemistry Analyzer, made in USA.6 Estimation of fasting Plasma glucose: Fasting plasma glucose (FPG) was measured by glucose oxidase – peroxidase method. using CobasMiras plus Automated Chemistry Analyzer, made in USA. 7 Estimation of HbA1c: HbA1c was estimated by turbidometric immunoassay method.8 Estimation of serum malondialdehyde: Serum malondialdehyde was estimated by thiobarbituric acid reactivity method.9 Clinical examination of Nervous system: Physical examination was done to assess motor and sensory nerve functions and deep tendon reflexes. Nerve Conduction Studies: Nerve Conduction Study examinations were performed according to the standard method recommended by the American Diabetes Association at 20 to 25°C room temperature. The velocity, amplitude, duration, F wave and latency was determined for peripheral nerves including. posterior tibial, peroneal, femoral, median, ulnar and sural nerves.Bilateral nerve conduction studies were performed for patients to improve the sensitivity of detecting possible mononeuropathy among them. Standard techniques of supramaximal stimulation with rings and surface recording electrodes were done for all participants. 10 Statistical Analysis: The data collected were entered and analyzed using software Statistical Package for the Social Science 16.0 (SPSS 16.0). All parameters were presented as mean ± standard deviation (mean ± SD). Comparison of parameters was done with student ‘t’ test. Correlation analysis was done with Pearson’s correlation method. A linear regression analysis was performed to evaluate the independent predictor of oxidative stress. A p value of less than 0.05 was considered statistically significant. RESULTS
Table 1: Comparison of various parameters between the cases and control group
Data are presented as Mean ±SD. * p<0.05 is considered statistically significant. MDA=Malondialdehyde, FPG=Fasting Plasma Glucose, GGT=Gammaglutamyl Transferase
Table 2: Correlation of GGT with various parameters among the cases
Pearson correlation analysis was performed to analyze the data. *p<0.05 is considered statistically significant. MDA=Malondialdehyde, FPG=Fasting Plasma Glucose, GGT=Gammaglutamyl Transferase.
Table 3: Correlation of GGT with various parameters among the controls
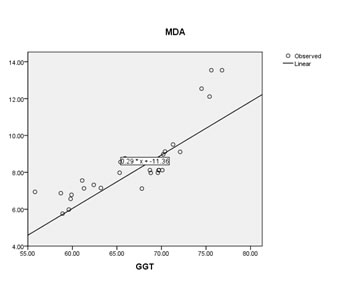
Pearson correlation analysis was performed to analyze the data. * p<0.05 is considered statistically significant. MDA=Malondialdehyde, FPG=Fasting Plasma Glucose, GGT=Gammaglutamyl Transferase Figure 1: Linear regression analysis between MDA and GGT levels among the cases The results were presented as mean ± standard deviation in table 1. The results showed that there is an increased serum GGT level in study group when compared to control group. Serum Malondialdehyde, fasting plasma glucose and HbA1c were significantly increased in the cases compared to the controls. There is significant association between raised GGT levels and fasting plasma glucose and HbA1c among the cases. Serum GGT was independently related with Malondialdehyde (MDA) according to linear regression analysis (P< 0.01).
DISCUSSION Diabetes mellitus is a metabolic disorder characterized by hyperglycemia. Hyperglycemia overloads glucose metabolic pathways, resulting in excess free radical production and oxidative stress in the peripheral nervous system and promote the development of diabetic neuropathy.11There are various proposed mechanisms for diabetic neuropathy, ranging from increased reactive oxygen species production, increased protein glycosylation, neurovascular disturbance, decreased neurotrophic support and possible role of inflammation.12,13 Oxidative stress, through the production of reactive oxygen species (ROS), has been proposed as the root cause underlying the development of insulin resistance, beta-cell dysfunction, impaired glucose tolerance and type two diabetes, it has also been implicated in the progression of long-term diabetes complications. Our study showed increased levels of serum GGT in patients with diabetic neuropathy. The primary function of GGT is to maintain the intracellular concentrations of glutathione (GSH), a critical antioxidant defence for the cell. So increased activity of GGT can be a response to oxidative stress, facilitating increased transport of GSH precursors into cells. In addition, GGT is leaked into the serum possibly because of various mechanisms such as increase in oxidative stress, proteolysis, glycosylation, and endothelial cell damage.14The serum levels of GGT also showed significant positive correlation with serum malondialdehyde, which is a biomarker of oxidative stress.This suggests that serum gamma glutamyl transferase (GGT) may be an early marker of oxidative stress that may contribute to the pathophysiology of the onset and progression of nerve injury in diabetic neuropathy through defects in metabolic and vascular pathways. The results are in accordance with a study by Whit field JB who reported that increased GGT activity may be a response to oxidative stress, which can increase the transport of glutathione precursors into cells.15 Gamma glutamyl transferase is an easy, universally standardized and routinely done test as part of liver function tests. Serum GGT is a useful marker for studying oxidative stress like serum MDA. Hence it can be used as a surrogate marker of microvascular complications in diabetes mellitus like diabetic neuropathy. Further studies using a larger sample size will be required to validate the results.
CONCLUSION The present study has shown that oxidative stress is associated with diabetic neuropathy. Poor glycemic control as reflected by increased HbA1c causes worsening of neuropathy. This study shows that increased levels of serum GGT may have important clinical implications in the presence of neuropathy in patients with type 2 diabetes. Serum GGT is a useful marker of oxidative stress in patients with diabetic neuropathy.
REFERENCES
|
|
 This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.